The Great COVID Death Coverup

Within weeks of the pandemic outbreak, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation was a death sentence; 76.4% of COVID-19 patients (aged 18 to 65) in New York City who were placed on ventilators died. Among patients over age 65 who were vented, the mortality rate was 97.2%
The recommendation to place COVID patients on mechanical ventilation as a first-line response came from the World Health Organization, which allegedly based its guidance on experiences and recommendations from doctors in China. But venting COVID patients wasn’t recommended because it increased survival. It was to protect health care workers by isolating the virus inside the vent machine
Data suggest around 10,000 patients died with COVID in NYC hospitals after being put on ventilators in spring 2020. Other metropolitan areas also saw massive spikes in deaths among younger individuals who were at low risk of dying from COVID. It’s possible many of these deaths were the result of being placed on mechanical ventilation
The WHO must be held accountable for its unethical recommendation to sacrifice suspected COVID patients by using ventilation as an infection mitigation strategy — especially considering they’re now trying to get unilateral power and authority to make pandemic decisions without local input
Showing how the WHO’s recommendation to put patients on mechanical ventilation resulted in needless death among people who weren’t at great risk of dying from COVID is perhaps one of the most powerful talking points a country can use to argue for independence and rejection of the WHO’s pandemic treaty
*
[embedded content]
Within weeks of the pandemic outbreak, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation was a death sentence.1
By early April 2020, many doctors were already questioning their use, as data2 showed 76.4% of COVID-19 patients (aged 18 to 65) in New York City who were placed on ventilators died. Among patients over age 65 who were vented, the mortality rate was a whopping 97.2%.
If you were older than 65, you were 26 times more likely to survive if you were NOT placed on a vent.3 A small study from Wuhan, China, put the ratio of deaths at 86%,4 and in Texas, 84.9% of patients died after more than 96 hours on a ventilator.5
In a widely-shared YouTube video6 (above) posted March 31, 2020, Dr. Cameron Kyle-Sidell, a critical care specialist at the Mount Sinai Health System in New York, warned that “we must change what we are doing if we want to save as many lives as possible.” Sidell was adamant that doctors were “treating the wrong disease” and that putting COVID patients on mechanical ventilation was all wrong.
“We are operating under a medical paradigm that is untrue,” Sidell said. “I fear that this misguided treatment will lead to a tremendous amount of harm to a great number of people in a very short time … This method being widely adopted at this very moment at every hospital in the country … is actually doing more harm than good.”
Why Were COVID Patients Put on Vents?
The recommendation to place COVID patients on mechanical ventilation as a first-line response came from the World Health Organization,7 which in early March 2020 published a COVID-19 provider guidance8 document to health care workers, based on experiences and recommendations from doctors in China.
According to the WHO, treatment needed to be rapidly escalated to mechanical ventilation. Ideally, patients should be placed on it immediately.9 What escaped the public was the primary reason why. Venting COVID patients wasn’t recommended because it increased survival; rather, it was to protect health care workers by isolating the virus inside the mechanical vent machine.
Using less invasive positive air pressure machines could result in the spread of infectious aerosols, the WHO warned. In other words, they put patients to death to “save” staff and other, presumably non-COVID, patients. That ventilation and sedation were used to protect hospital staff was highlighted by The Wall Street Journal in a December 20, 2020, article,10 which noted:
“Last spring, doctors put patients on ventilators partly to limit contagion at a time when it was less clear how the virus spread, when protective masks and gowns were in short supply.
Doctors could have employed other kinds of breathing support devices that don’t require risky sedation, but early reports suggested patients using them could spray dangerous amounts of virus into the air, said Theodore Iwashyna, a critical-care physician at University of Michigan and Department of Veterans Affairs hospitals in Ann Arbor, Mich.
At the time, he said, doctors and nurses feared the virus would spread through hospitals. ‘We were intubating sick patients very early. Not for the patients’ benefit, but in order to control the epidemic and to save other patients,’ Dr. Iwashyna said. ‘That felt awful.’”
As dryly noted by James Lyons-Weiler in a January 23, 2023, Substack article,11 “euthanizing humans is illegal. Especially for the benefit of other patients. It should feel awful.”
Fauci Knew Vents Did More Harm Than Good
[embedded content]
Even Dr. Anthony Fauci, in a mid-June 2022 lecture (above), admitted that placing patients on mechanical ventilation did more harm than good.
“We very, very readily would put people on mechanical ventilation, when we found out, through clinical experience, it might have been better just to make sure we positioned them properly in the prone or supine position, and not necessarily to intubate someone so readily, which might have actually caused more harm than good. We learned that as we got more experience.”
Yet government treatment guidelines, to this day, include invasive mechanical ventilation.12 If the White House Coronavirus Task Force knew in the summer of 2022 that venting patients caused more harm than good, why didn’t they instruct hospitals to stop using it? Or at bare minimum, strongly advise against it?
And why did the government continue to financially incentivize the use of mechanical ventilation after they’d realized how bad it was? While many hospitals did cut down on their use of mechanical ventilation toward the end of 2020 and beyond, it still hasn’t been entirely replaced with noninvasive strategies shown to be far more effective.13
Many ‘COVID Patients’ Didn’t Have COVID
The matter becomes even more perverse when you consider that many “COVID cases” were patients who merely tested positive using faulty PCR testing. They didn’t have COVID but were vented anyway, thanks to the baseless theory that you could have COVID-19 and be infectious without symptoms.
Hospitals also received massive financial incentives to diagnose patients with COVID — whether they had it or not — and to put them on a vent. They also received bonuses for using toxic remdesivir, and they were paid for each COVID death as well. The entire system was set up to reward hospitals for misdiagnosing, mistreating and ultimately killing patients.
China also benefited from the WHO’s misguided advice. While the U.S. clamored for more ventilators, Chinese hospitals started relying on them less and instead they were being exported in huge quantities.14
How Many COVID Patients Were Killed by WHO’s Bad Advice?
Just how many COVID-19 patients were killed by being placed on mechanical ventilation in the spring of 2020? That’s a question attorney and author Michael P. Senger tries to answer in his May 25, 2023, article “The Great COVID Ventilator Death Coverup.”15 He writes, in part:
“… the establishment is trying to argue that while ventilators were overused in spring 2020, doing more harm than good … the ventilators themselves did not kill anyone.16 An astonishing argument, even by the abysmal standards of the COVID era.
But, since everyone supporting this narrative is arguing that there were no ventilator deaths in spring 2020, all we have to do is prove there were a significant number of ventilator deaths and what’s left of the establishment’s credibility on the initial months of COVID falls apart.
In addition to the anecdotal evidence … several unsettling data points have long strongly suggested that there weren’t just some ventilator deaths in spring 2020, but rather a pretty frightening number of them …
The CDC reports17 that 18,679 patients died with COVID in New York City hospitals throughout spring 2020. And, according to the sample in JAMA,18 just over half of those who died with COVID in NYC hospitals were put on ventilators. Accordingly, around 10,000 patients died with COVID in NYC hospitals after being put on ventilators in spring 2020 …
Additionally, as Jessica Hockett has documented19 in meticulous detail through multiple methods, New York City experienced a sharp, breathtaking mortality event just after its lockdown and response to COVID began, which was unlike that experienced anywhere else or at any other time.
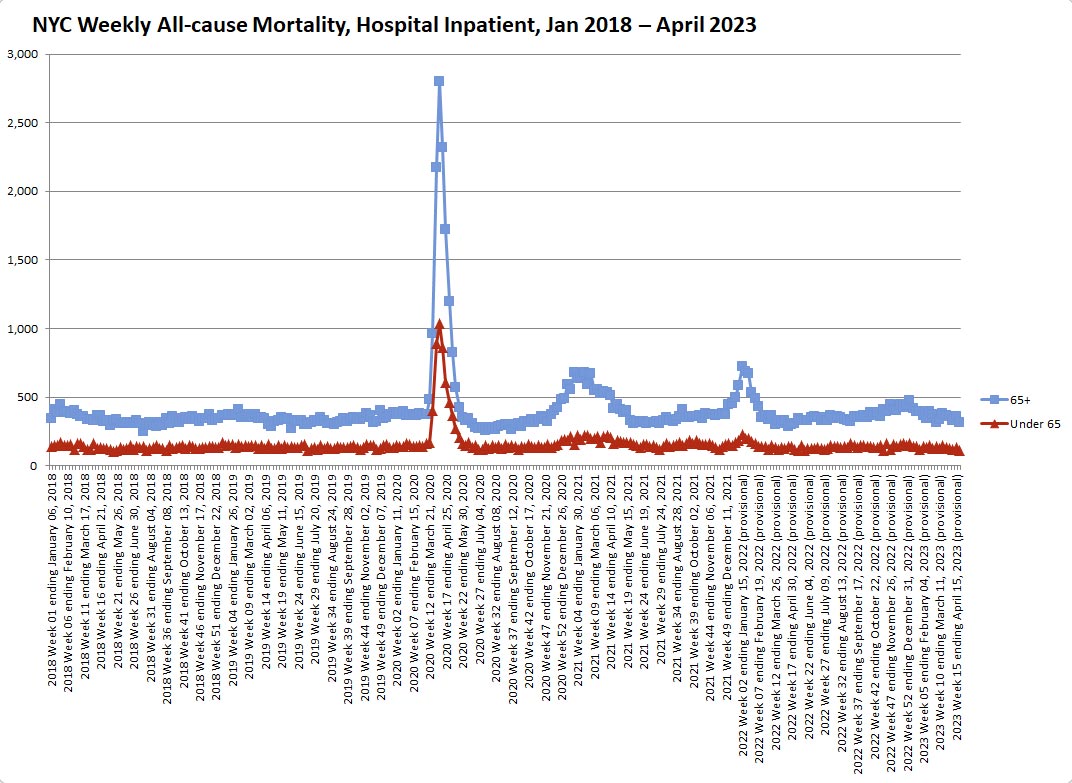
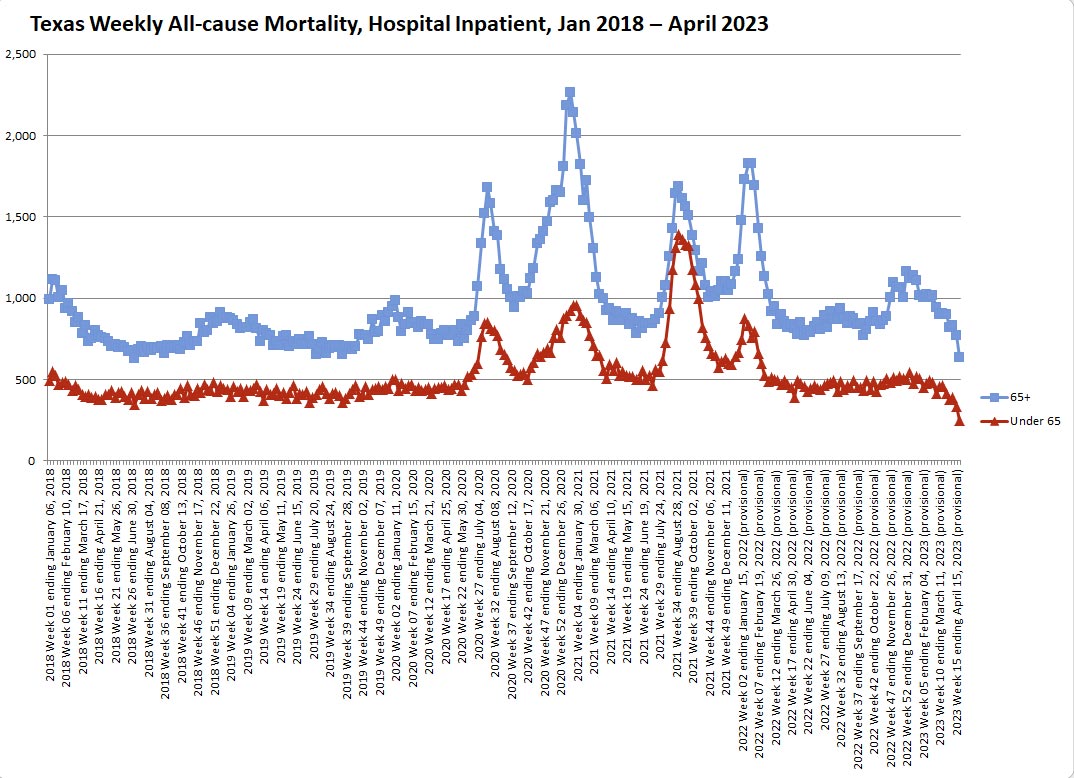
Given its singularity, this horrifying mortality event, quite simply, cannot be attributed to natural causes. Jumping off Hockett’s work, below is a chart of weekly all-cause hospital inpatient mortality from January 2018 through April 2023, split between patients ages 65+ (blue line) and patients under 65 (red line).
This spike in inpatient hospital mortality in New York City in spring 2020, especially among young people, is unparalleled in any other time period, even as COVID deaths supposedly began to climb again in 2021.”
Inpatient Mortality Around the US, 2020 Through Present
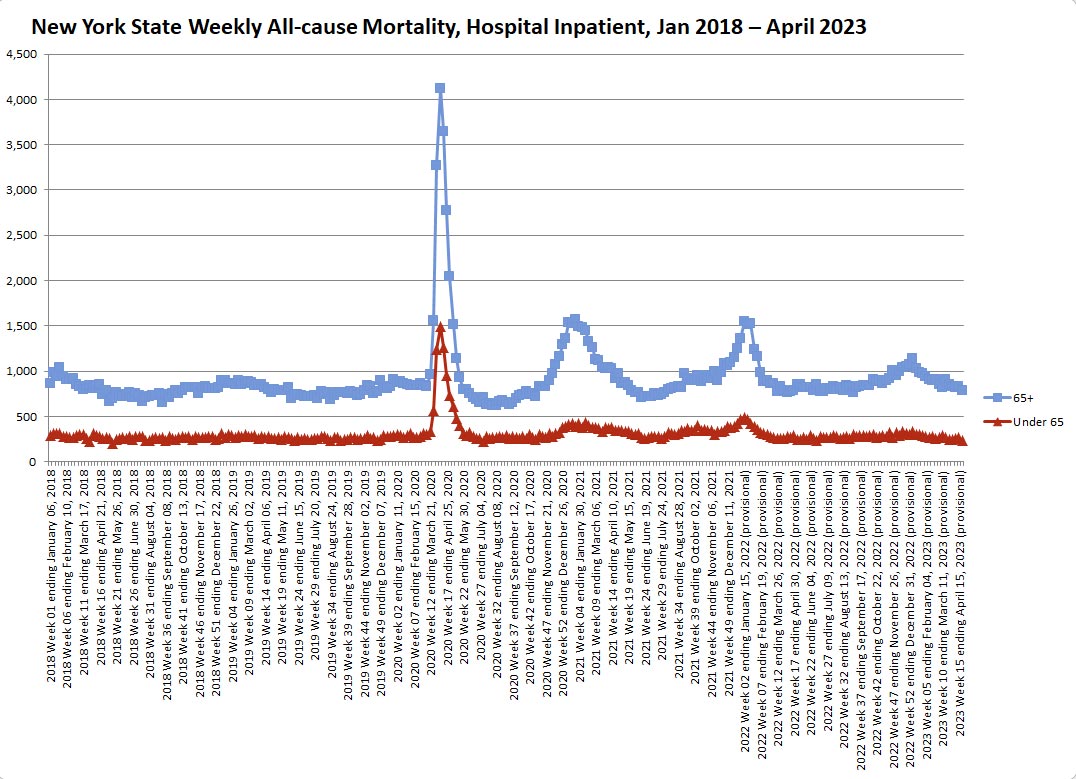
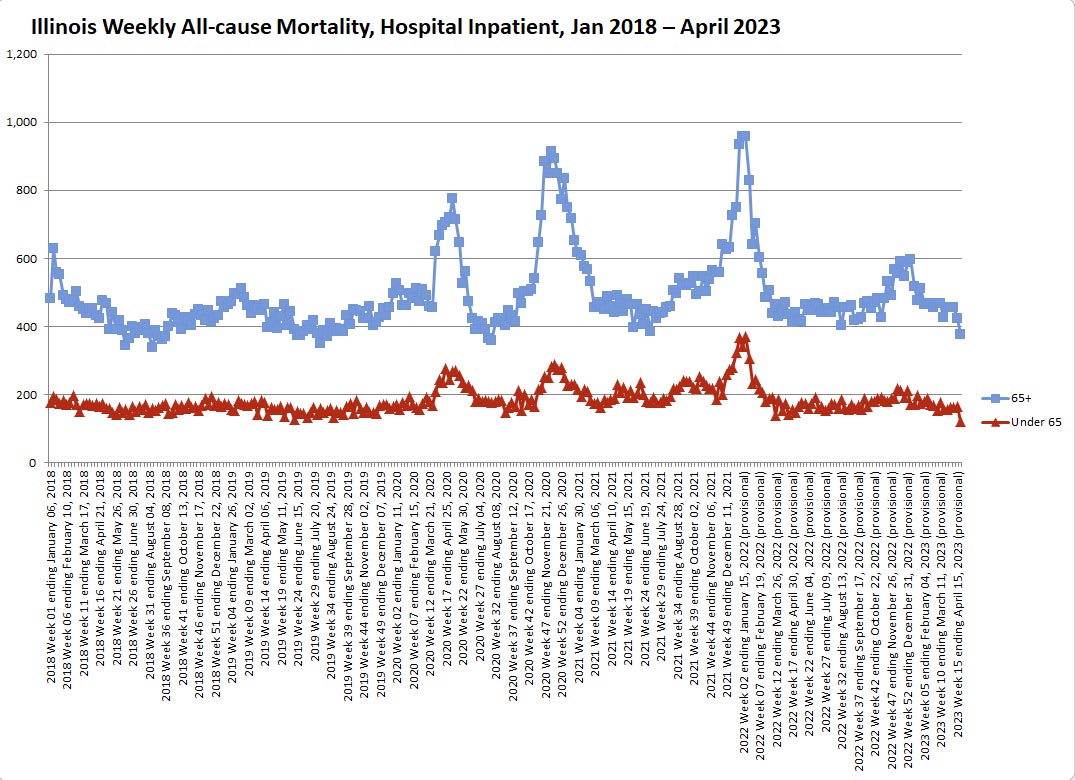
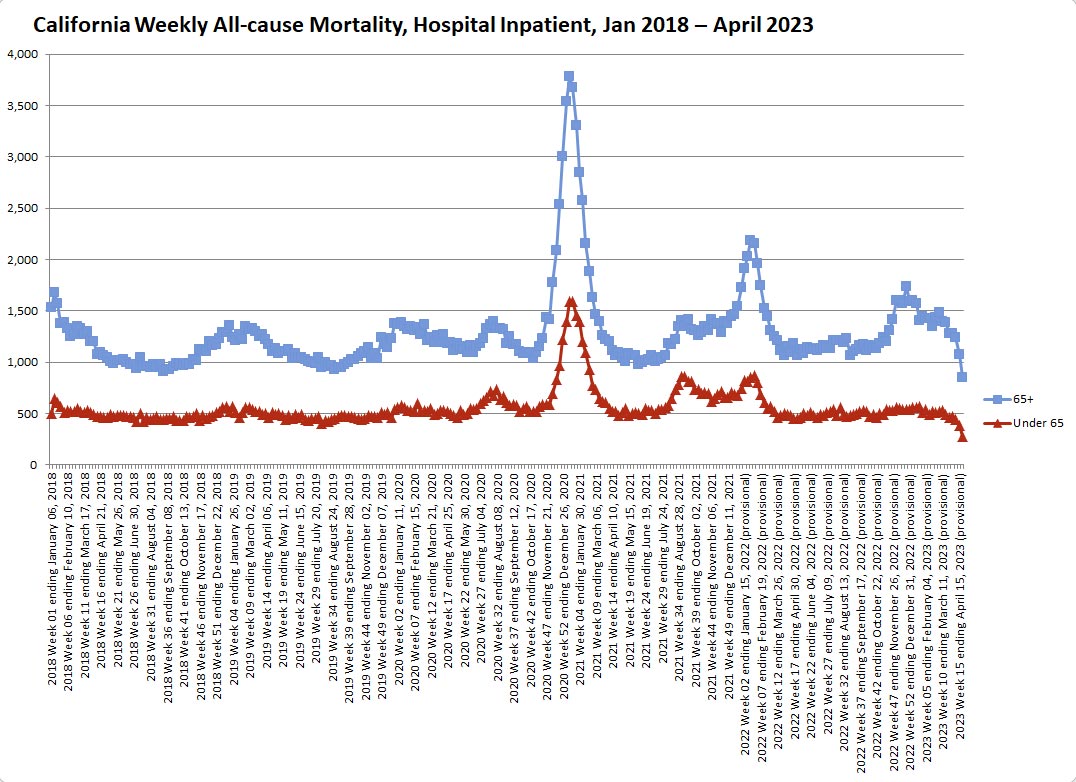
Senger goes on to show the same all-cause mortality graphs for hospital inpatients for each of the largest cities in the U.S.: Chicago, Dallas, Houston, Los Angeles and Washington, D.C. All show massive spikes in hospital deaths, especially among the elderly (65 and older), around the same time periods as NYC. He also produced charts for deaths on the state level, as follow:20
A Strawman Argument
Senger continues:21
“A couple of points on these charts. First, while the spike in mortality in the NYC area in spring 2020, especially among young people, is without parallel, it’s not the only one we see.
These spikes in mortality among young people are conspicuous because it’s long been known that COVID’s infection fatality rate (IFR) is extremely skewed toward the elderly. This, for example, is the most widely-cited data on COVID’s IFR by age:22
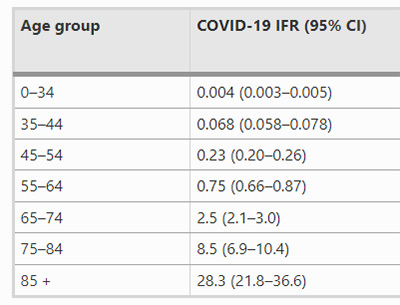
Thus, these spikes in mortality among young people cannot be attributed to COVID. Most notably, a significant spike in mortality appears among all age groups in California at the end of 2020 …
One possibility is that, while the use of ventilators was generally scaled back, hospitals in California may have still been engaging in broad intubation or other iatrogenic practices by the end of 2020 …
Even more strangely, Texas experienced a surge in deaths among young people in summer 2021 that was not accompanied by a corresponding increase in mortality among the elderly; this, frankly, may have had nothing to do with COVID.
That said, the fact remains that the New York area experienced a uniquely sharp, awful mortality event in spring 2020 which is not adequately explained by any of these other factors.
And doctors were under significant pressure to put patients on ventilators in spring 2020, even if it was merely unconscious; politicians had purchased tens of thousands of ventilators at exorbitant prices, and hospitals did receive more funding if patients were placed on ventilators.
Coupled with the above anecdotes about patients being placed on ventilators for extended periods to protect staff — and the fact that over 10,000 patients in New York City died after being intubated — it’s clear that a horrifying number of patients were likely killed by mechanical ventilators.
Yet astonishingly, despite all these facts, the establishment is arguing that no patients were killed by ventilators in spring 2020. This, to me, is the kind of implausible, overly-defensive argument one makes when they’re panicked.
Across America, tens of thousands of patients were placed on ventilators in spring 2020; given the vast majority of those patients died, it simply begs credulity that none of them were killed by ventilators.
When a deadly procedure is applied to tens of thousands of patients, even a baseline level of human error would imply that the procedure was applied to at least some fraction of those patients by mistake.
The establishment has responded with subsequent studies23 claiming to show that ‘early intubation’ actually reduced the time patients spent on ventilators, and thus didn’t kill any of them. But this is a straw-man argument …
[T]he issue isn’t whether patients were intubated ‘early’ or ‘late’ relative to any symptoms they might have shown — the issue is whether patients were placed on ventilators who should have never been on them to begin with, or otherwise kept on them too long.”
A Morally Indefensible Coverup
Senger points out that, in speaking with other attorneys, most agree that hospitals face virtually no risk of litigation over ventilator deaths, for the simple reason that everyone perceived COVID to be a global emergency, and during emergencies, you just do the best you can with what you have and what you know.
“Regardless of how much harm was done, it’s simply too difficult to prove that the procedure violated the emergency standard of care given the information coming from China at the time,” he writes.
Even so, “the situation is morally inexcusable,” Senger says, adding that we do need to get to the bottom of how and why these patients died. I agree. While Senger wants the truth to understand what happened and to honor the diseased, I would add that we need the truth in order to avoid making the same mistake again, because there will be a next time.
The WHO Must Be Held to Account
The WHO must be held accountable for its unethical recommendation to sacrifice suspected COVID patients by using ventilation as an infection mitigation strategy — especially considering they’re now trying to get unilateral power and authority to make pandemic decisions without local input.
Showing how the WHO’s recommendation to put patients on mechanical ventilation resulted in needless death among people who weren’t at great risk of dying from COVID is perhaps one of the most powerful talking points a country can use to argue for independence and rejection of the WHO’s pandemic treaty.
They simply cannot be trusted to make sound medical decisions for the whole world. No one is. We need to allow local medical experts to make the calls in situations like this, and to collaborate and share information between themselves. The top-down one-size-fits-all medical paradigm that the WHO wants to implement is nothing short of disastrous, and the COVID pandemic response proves it.
Also, let’s not forget that the misuse of mechanical ventilation created the appearance that COVID was exceptionally deadly, regardless of your age, which in turn helped promote acceptance of the experimental COVID shots that are now a leading cause of frequent sickness, chronic disability and excess deaths. Of course, that’s also being covered up.
In the final analysis, the WHO’s handling of the COVID pandemic will undoubtedly go down as the worst in medical history. Can we really trust them to make better decisions in the future?
I think not, which is why we must do everything in our power to prevent the U.S. from signing the pandemic treaty. Better yet, we need to exit the WHO entirely. To that end, I urge you to contact your local House representatives and Senators and urge them to:
- Support the No WHO Pandemic Preparedness Treaty Without Senate Approval Act24,25,26,27,28
- Withhold funding for the WHO
- Support U.S. withdrawal from the WHO
*
Note to readers: Please click the share button above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Notes
2 JAMA April 22, 2020; 323(20): 2052-2059 Outcomes for Patients Who Were Discharged or Died
3, 15, 20, 21 Michaelpsenger.com May 25, 2023
4 The Associated Press April 8, 2020
5 Citizens Journal December 20, 2021
6 YouTube Cameron Kyle-Sidell March 31, 2020
7 The Dossier Substack September 30, 2020
8 WHO Clinical Management of Severe COVID-19
9 WHO Infection Prevention and Control for COVID
10 Wall Street Journal December 20, 2020
11 Substack Popular Rationalism January 23, 2023
12 NIH Covid Treatment Guidelines Updated April 20, 2023
17 CDC MMWR November 20, 2020; 69(46): 1725-1729
18 JAMA April 22, 2020; 323(20): 2052-2059
19 Woodhouse Substack April 18, 2023
22 European Journal of Epidemiology 2020; 35: 1123-1138
23 Science Based Medicine September 19, 2021
24 Tiffany.house.gov March 7, 2023
25 No WHO Pandemic Preparedness Treaty Without Senate Approval Act House Bill Full Text
26 Congress.gov S.4343 — No WHO Pandemic Preparedness Treaty Without Senate Approval Act
27 Congress.gov S.444 — No WHO Pandemic Preparedness Treaty Without Senate Approval Act
28 Govtrack.us S.4343 — No WHO Pandemic Preparedness Treaty Without Senate Approval Act
Featured image is from Mercola

