The US nursing home data is devastating for the narrative; now it’s time for our own peer review before we submit this to a journal
Guest Post by Steve Kirsch
From the US Nursing home data, we can now prove that the vaccines increased the odds of death from COVID by 6%. I need 20 data scientists to validate my work before I submit to a journal.
Executive summary
The US nursing home data shows that the COVID vaccines increased the odds of death from COVID by 6%. The result is highly statistically significant.
Emory University infectious disease Professor Carlos del Rio reviewed my work, thought it was flawed, and encouraged me to submit it to a peer-reviewed journal where he presumed it would be rejected.
When prompted, he was unable to articulate a single flaw and refused to talk to me.
So I’m going to follow his advice.
But before I attempt that, I want to make sure I have at least 20 peer reviewers who have reviewed my work. If there is a mistake, I want to find it before I submit it to the journal. I want to make sure this is bulletproof so that the journal will not have any excuses for rejecting this important result.
If you are a data scientist or epidemiologist who is willing to verify my result, this would be extremely helpful. Please sign up here.
Data source
US Nursing home data collected by CMS from 15,410 providers who submit COVID cases and deaths within their facility weekly since week ending 5/24/20.
This is the most comprehensive dataset on the single most important demographic for COVID:
- More than 40% of the COVID deaths were from nursing homes in the beginning of the pandemic.
- Older adults made up 90% of US COVID deaths in 2023
So if the COVID vaccine was or wasn’t effective for this group, this data would tell the story.
This data is also the most credible because there were over 15,000 independent observers. So we can look at the aggregated results while minimizing any systematic errors as might occur if the numbers were collected by a single entity.
Methods
I downloaded the raw data from the site (the .csv files). The data was processed using an R program.
The code and data analysis can be found in my github repo for this project. Everything was done in public view.
The code does the following:
- Reads in the .csv files
- Computes summary statistics for each nursing home
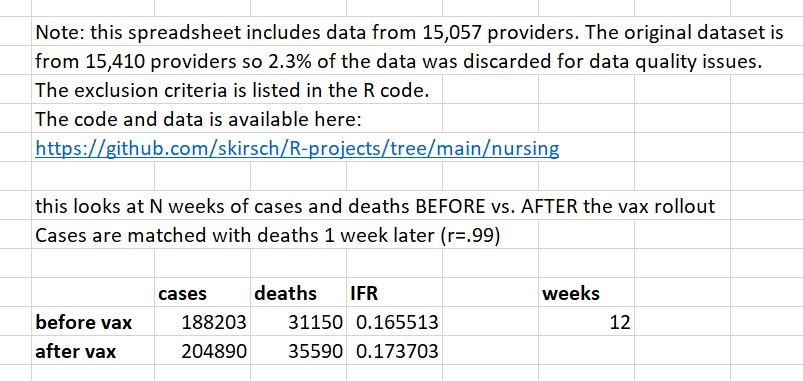
- Uses the stats in a set of QA checks. Then discards all data from those nursing homes with nonsensical aggregate results (e.g., deaths > cases). This resulted in the elimination of all data submitted by 2.3% of the nursing homes.
- Sums up the COVID cases and deaths for each week from all the remaining nursing homes.
Then using an excel spreadsheet, I summed the cases and deaths for N weeks before vs. after the vaccine rollout, using a 1 week delay for cases as per the work done by Mike Deskevich.
I looked at various values of N, with N=12 being the most reasonable to detect an effect. For all values of N between 1 and 24, the result showed that the vaccine increased the risk of death.
I used a demarcation date of the week ending 12/6/20 as the pre-vax period. The Excel spreadsheet (see the week tab in the top right) allows you to vary this and it didn’t change the result if you moved it later, e.g., by 3 weeks since the vaccination rollout was widespread by 12/27/20. In fact, it made the disparity worse for those claiming the vaccine reduced death (RR=1.066 vs. RR=1.049 for demarcation week offset=0).
Additional evidence relevant to the nursing home data
- All this data has been available publicly for at least 2 years. If the data showed the vaccines worked, why isn’t there a publication showing us that the IFR decreased. There are a few paper referencing this nursing home dataset which you can find here:
- Nursing Home Resident and Staff Covid-19 Cases After the First Vaccination Clinic which looks at cases, but NOT the IFR! The problem is that cases come and go and people falsely associate the going with the vaccine rollout.
- <more added shortly>
- It seems that some people believe that this is a CFR and not an IFR because nursing homes didn’t test everyone every day. Nursing homes only tested symptomatic people. The deaths/cases ratio here is about as close to an IFR as you can get. A CFR is applicable to large populations where 100% of the population who is symptomatic cannot be centrally screened. By contrast, nursing homes are closed environments where if you are sick, the staff notices. Also, the testing policy (test residents who exhibit symptoms) never changed over the period (no new instructions from Medicare or the CDC).
- Nobody who discounted my analysis was able to articulate what the “correct” IFR was prior to the vaccine rollout. They all avoided answering the question. If you don’t know what the right answer is, how can you be certain that the reported data is wrong? The answer is simple: you can’t.
- Professor Jeffrey Morris’s critique is that 1) you don’t have infections and deaths for the same cohort and that 2) the data doesn’t include the vaccination status of the infected and dead. He says that because of those two things, you cannot publish any paper making any kind of observations about the data. That is simply stunning. The corollary is that all ecological studies ever done should be retracted by every journal; for example studies saying highly vaccinated countries have lower mortality should be retracted because you don’t know the vaccination status of the dead.
- The IFR matches numbers found in peer-reviewed studies. The John Ioannidis paper, Infection fatality rate of COVID-19 in community-dwelling elderly populations, says “Median IFR in all elderly for all 11 high-income countries was 4.5% (range 2.5–16.7%).” We found an IFR in the nursing homes of 16%. But the nursing homes only tested symptomatic patients. Nearly 78% of original strain COVID infections are asymptomatic so that means our 16% should be reduced by a factor of 4.5 to get the true IFR (our IFR was calculated based on symptomatic cases). 16%/4.5=3.5% so we are squarely in the range of the Ioannidis paper. Since we are under the median IFR, it means that we are not “missing” tracking any significant number of cases (see Limitations section), i.e., if there were missing cases that we weren’t seeing, this would lower our IFR even more and it is already well within the expected range.
- This JAMA paper, Infections, Hospitalizations, and Deaths Among US Nursing Home Residents With vs Without a SARS-CoV-2 Vaccine Booster, shows a VE of 87.9% in System 1. So that’s comparable to the NSW claims. So if the vaccine really did that, the effect would be easy to spot in the US Nursing home data. It’s impossible to spot. Also, that paper shows that the booster shots take effect almost instantly since you can see from Figure 1C that the slope difference between boosted vs. unboosted is dramatically different on Day 7 after the shot. But a booster provides nearly no benefits as we can see in our data, so that means that the effect of the primary series should be even more dramatic. By day 7. So this means that certainly by Feb 7, 2021, which is well after half the nursing home population is fully vaccinated (see chart below), we’d see a huge IFR reduction vs. baseline. Baseline IFR on 12/6/20: 0.171526 Feb 7, 2021 IFR: 0.17958. There was no reduction. It actually increased! Maybe we should wait 30 days after the nursing homes had half the residents who were fully vaccinated. OK. On March 7, 2021, the IFR value for the week was 0.219485. Even worse! This is a HUGE HUGE problem.
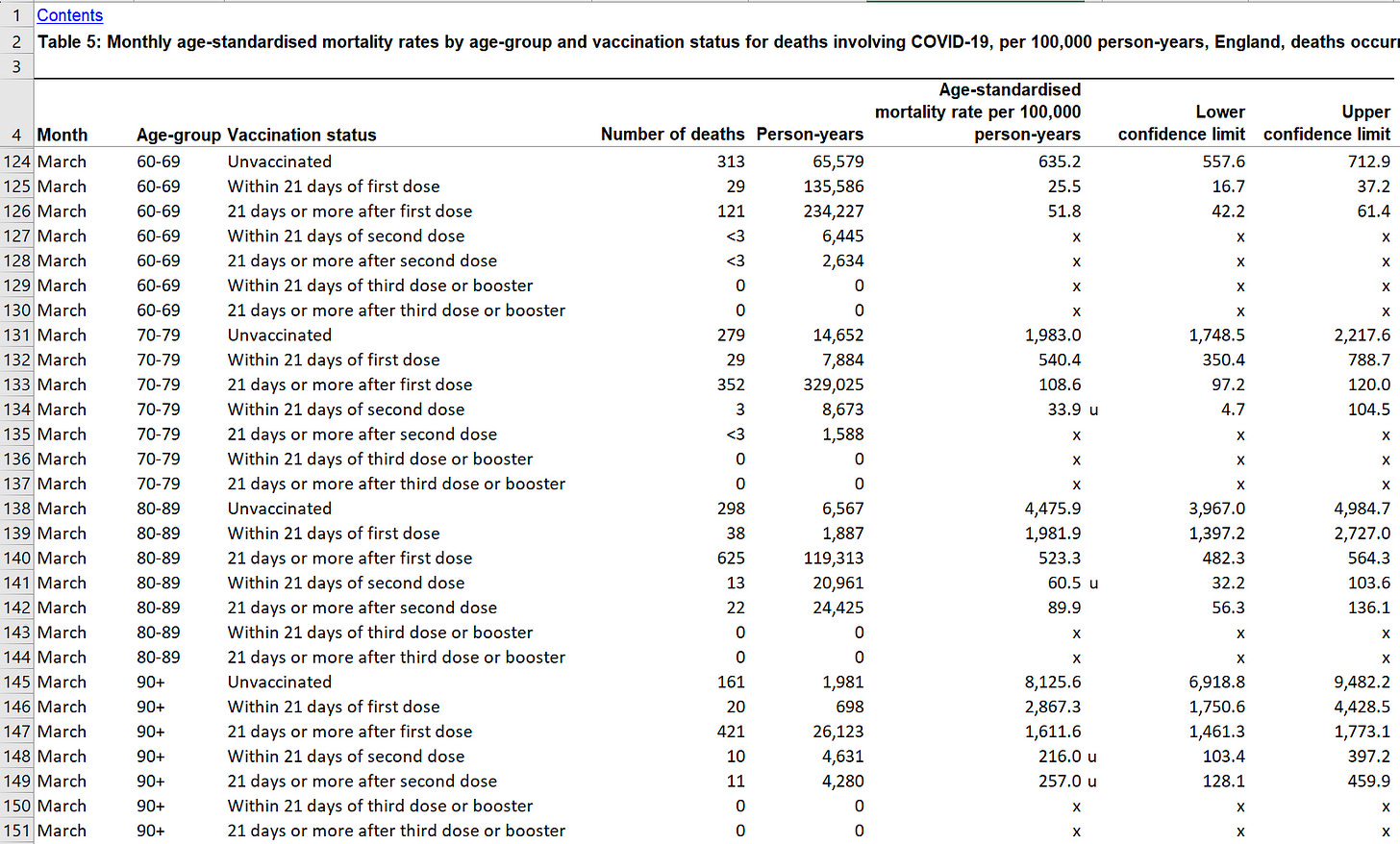
- Note that the UK data also claims that the vaccine “works” very rapidly, certainly within 21 days of the first dose. Download the UK ONS data here. Here’s a snippet showing HUGE reductions in COVID mortality just 21 days after the first shot. For example, a 60 year old goes from an ASMR for COVID of 635 per 100K person-years to just 25.5, which is a reduction of 25X (but they are 95% confident it’s at least a 15X reduction (557/37). That’s just after the first dose. Can you imagine what the reduction after the second dose must be! It’s so high they can’t even measure it!!! So we should be seeing HUGE IFR reductions in the data 30 days after 50% of the population is fully vaccinated, right?. But as I noted above, the IFR increased from .17 (baseline) to .22 (March 7, 2021), which is a 29% increase. That is a HUGE HUGE problem.
-
UK ONS data shows the vaccine drops COVID mortality for 60-69 year-olds by at least a factor of 15X within 21 days of the very first dose! - The probability density function (histograms on the Provider tab of the spreadsheet) matches a Poisson distribution. This is a good sign the data reflects what we think it reflects.
- Nearly 60% of the elderly in nursing homes had one dose by Jan 3, 2021 and two doses by Feb 14. So our 12 weeks analysis from 12/6/20 included data until March 7, 2021. Even analyses further out (16, 20, 24) showed the IFR was still elevated. That simply can’t happen if the vaccine reduces death. The IFR is naturally declining and if the vaccine worked, it would turbo charge this natural reduction and we’d see a huge signal. We don’t. The huge signal we do see is when Omicron hits; it’s unmistakable.

Limitations
In all the nursing homes I am aware of, all newly admitted residents and all symptomatic patients are tested for COVID.
Some people have suggested that nursing homes were expressly told not to count infections of newly admitted residents
The data dictionary doesn’t mention this as a factor. If this were material, they would have mentioned it in the data dictionary.
Nor did the reporting instructions (the Interim Final Rule Updating Requirements for Notification of Confirmed and Suspected COVID-19 Cases Among Residents and Staff in Nursing Homes) mention that nursing homes should not count such cases.
They told people the vaccines reduce your risk of death by 10X. It did no such thing.
They told people that the COVID vaccines would reduce the risk of death by 10x.
For example,

Here’s the death image (lower right in the tweet) showing the 10X reduction:

Reality: It increased your odds of death from COVID by 6%
If we do a Fisher Exact Test to see if this is statistically significant and to look at the confidence intervals, we see the result is highly statistically significant.
Note that the odds ratio (OR) and relative risk (RR) are similar but computed different ways (one using number dead:survive and the other using IFR ratios) so they will always differ:
Statistics for Nursing home 12 week case
- Fisher Exact Test parameters: 157053 169300 31150 35590
- One-sided p-value: 4.236409729747196e-12
- Odds ratio= 1.059
- 95% Confidence Interval: 1.042 to 1.078
In plain English, there was a 6% higher odds of death in the 12 week period post-vaccine vs. a 12 week period pre-vaccine in the nursing homes.
This is a devastating result. It shows that the US government forced people to take a vaccine that would increase their risk of death from COVID.
An earlier paper showed that the COVID vaccine also increases your risk of getting COVID.
In short, the COVID vaccines were all risk and no benefit.
If the vaccines worked, it would show up in the US Nursing home dataset
If the vaccines worked as promised (a 10X reduction in death as claimed by certain health authorities), the very first place you’d see a huge and clear benefit would be in this data.
You don’t. You see the opposite: a rise in the risk of death on the same variant as before the vaccines were rolled out (so it wasn’t the variant).
All in all, the COVID vaccines were the deadliest medical interventions in US history.
The consistency of the data
If you look at the 1 week before vs. after analysis of the dataset, the numbers are nearly identical. But as the weeks increase, the differences are apparent.
If you look at the 24 week period before the vaccine rolled out, the second 12 weeks had a lower IFR than the first 12 weeks. This is exactly as expected as the IFR gradually drops over time (more people have been infected once already so on the second time, it’s a lower death risk, dry tinder has been burned).
Note also that when averaged over a few weeks or more, the IFR is quite stable (see the various analyses in the weeks tab on the spreadsheet; I compute for 1,4,8,12,16, and 24).
If you are in the same variant, the only thing that can cause a rise in the IFR of a virus is human intervention. That’s exactly what we have here.
Summary
This is official US government data and the single most complete and trusted dataset for what happened at US nursing homes before and after the vaccine.
The IFR should have dropped like a rock after the vaccines rolled out. But instead the odds of death increased by 6%. Furthermore, the odds of death did drop like a rock later, right when Omicron rolled out; exactly as predicted.
This is a devastating result that shows that most of the doctors and health authorities ended up recommending a medical intervention that killed people.
To make this as solid as possible, I want to have at least 20 highly qualified peer reviewers. Please sign up here. This work has already been reviewed by others including Norman Fenton who praised it.


