The Evidence – You stayed at Home, to protect the NHS, but they gave Midazolam to the Elderly and falsely told you they were COVID-19 Deaths

In March 2020 the British people were told that they must “stay at home” in order to “protect the NHS” and “save lives”. They were also told that the authorities needed just “three weeks to flatten the curve”.
Why were the British people instructed to stay at home? Because of the threat of a new and emerging virus which we’re told originated in the city of Wuhan, China. A virus which has claimed the lives of 128,000 to date in the United Kingdom, or so we’re told.
But what if we could prove to you that you’ve given up fifteen months and counting of your life due to a lie? But not just any lie, a lie that has involved prematurely ending the lives of thousands upon thousands of people, who you were told died of Covid-19. A lie that has involved committing one of the greatest crimes against humanity in living memory. A lie that has required three things – fear, your compliance, and a drug known as Midazolam…
Let’s not lose touch…Your Government and Big Tech are actively trying to censor the information reported by The Exposé to serve their own needs. Subscribe now to make sure you receive the latest uncensored news in your inbox…
Authorities state that Covid-19 is an infectious disease caused by a new coronavirus dubbed SARS-CoV-2. The World Health Organisation (WHO) tell us that “most people infected with the COVID-19 virus will experience mild to moderate respiratory illness and recover without requiring special treatment”. However they state that “older people, and those with underlying medical problems like cardiovascular disease, diabetes, chronic respiratory disease, and cancer are more likely to develop serious illness”.
We’re told that serious illness in Covid-19 presents pneumonia and accompanying respiratory insufficiency. Therefore typical symptoms include breathlessness, cough, weakness and fever. We’re also told that people who suffer deteriorating respiratory failure and who do not receive intensive care, develop acute respiratory distress syndrome with severe breathlessness.

Pneumonia is an inflammation of one or both lungs, usually caused by an infection. It causes the alveoli (air sacs) inside the lungs to fill with fluid, making it harder for them to work properly. The body sends white blood cells to fight the infection, and while this helps kill the germs it can also make it harder for the lungs to pass oxygen into the bloodstream.
Pneumonia is not a new condition that has appeared due to Covid-19. In 2019 alone, the year prior to the alleged emergence of Covid-19, 272,000 people were admitted to hospital with pneumonia. According to the British Lung Foundation in 2012, 345 people per every 100,000 had one or more episodes of pneumonia. This equates to around 225,000 people suffering pneumoni at least once.
The British Lung Foundation also show us that the majority of cases of pneumonia occur in those who are aged 81 and over. For instance in 2012 1,838 people in every 100,000 people over the age of 81 developed pneumonia, this equates to around 60,000 people over the age of 81 in today’s numbers based on there being around 3.2 million people over the age of 80 in the UK.
They also tell us that In 2012 there were 28,592 deaths from pneumonia, which equates to 5.1% of all deaths that occurred that year.

So as you can see deaths due to pneumonia have not just suddenly started to happen because of the alleged emergence of a new disease called Covid-19, we’ve been living with them all of our lives, they just haven’t been thrust in front of you 24/7 on the television, or the front page of every newspaper like they have with alleged Covid-19 deaths.
But for us to prove to you that you given up fifteen months of your life due to a lie that involved prematurely ending the lives of thousands upon thousands of people we first need you to understand which age group has been most affected by Covid-19 according to official statistics.

The above graph is a heat map showing deaths within 28 days of a positive test for SARS-CoV-2 by date of death and age of the person. This data can be seen at the UK Gov’s. coronavirus dashboard here. Whats pretty clear from this data is that the most alleged Covid deaths have occurred in people aged 90+. The next age group with the most deaths being 85 – 89, then 80 – 84 and so on and so on. There’s a general decrease in the number of deaths up to about the 65-69 age group but then we see a dramatic fall to pretty much zero in anyone aged under about the age of 60.
This heat map shows that there have generally been no more than 9 deaths in a single day of anyone aged between 60 – 64. In the 65-69 year old group there have been no more than 20 deaths a day. In the 70-74 year old group no more than 27 deaths in a day. In the 75-79 group no more than than 48 deaths in a day, at it’s highest. It isn’t until we get to the 85-89 year old group that we start to see a large increase in the number of alleged Covid deaths. 179 deaths in a day at its highest. Then we have the 90+ age group which has seen no more than 379 deaths in a single day at it’s highest.
So what we’re seeing here is that is a negligible amount of “Covid” deaths in anyone under the age of 60. But we’re really not seeing very many “Covid” deaths in anybody aged between 60 and 80. What we are seeing is a much higher amount of “Covid” deaths in people aged over 85. But what’s so strange about that?
Well nothing when we consider the average life expectancy in the UK is 81 years of age. Plus the fact this is also in line with what we have seen in cases / deaths due to pneumonia in previous years. Don’t forget serious illness in Covid-19 presents pneumonia and accompanying respiratory insufficiency.
Which begs the question of why the entire nation has had to stay at home, social distance, wear a mask, wash their hands, and live under dictatorial tyranny for fifteen months because people who have lived longer than the average life expectancy in the UK have died or are dying? Dying of pneumonia from which we see tens of thousands of deaths every year.
We cannot deny that 2020 did see excess deaths, and you would believe this is due to the hospitals being overwhelmed? Except they weren’t.
NHS data shows us that during the height of the “first wave” between April and June 2020 there were 58,005 beds occupied which equated to 62% occupancy. This is 30% down on the same time frame in the previous year.

- In 2017, April-June there were on average a total of 91,724 beds occupied which equated to 89.1% occupancy.
- In 2018, April-June there were on average a total of 91,056 beds occupied which equated to 89.8% occupancy.
- In 2019, April-June there were on average a total of 91,730 beds occupied which equated to 90.3% occupancy.
- In 2020, April-June there were on average a total of 58,005 beds occupied which equated to 62% occupancy.
It also shows us that A&E attendance during the height of the first wave was 57% down on the previous year.

- 2018 – April – 1,984,369 attended A&E
- 2019 – April – 2,112,165 attended A&E
- 2020 – April – 916,581 attended A&E
Which begs the question of what exactly were we protecting the NHS from? It seems to have had a holiday.
But there were 41,627 more deaths than the five year average up to the 1st May 2020, and the vast majority of these occurred in April. An April which saw A&E attendance down 57% compared to the previous year and bed occupancy down 30% compared to the previous year. 33,408 of these excess deaths mentioned Covid-19 on the death certificate, the vast majority of which occurred in those over the age of 85.

However data taken from the Office for National Statistics (ONS) shows us that during April 2020 there were 26,541 deaths that occurred in care homes, an increase of 17,850 on the five-year average. This is half the amount of alleged Covid-19 deaths during the same period.

Why did so many people die in care homes when hospitals were far from overwhelmed? Surely if they have developed serious complications due to Covid-19 they would require urgent medical attention and hospital treatment?
Because don’t forget we’re told that serious illness in Covid-19 presents pneumonia and accompanying respiratory insufficiency. Therefore typical symptoms include breathlessness, cough, weakness and fever. We’re also told that people who suffer deteriorating respiratory failure and who do not receive intensive care, develop acute respiratory distress syndrome with severe breathlessness.
Why were these people in care homes and not in hospital?
They were in care homes because Matt Hancock gave the order to put them there…

On the 19th March a directive was sent out to the NHS which required them to discharge all patients who they deemed to not require a hospital bed. They declared that transfers from the ward must happen within one hour of that decision being made to a designated discharge area, and that discharge from hospital should happen within 2 hours. NHS trusts were told that “they must adhere” to the new directive.
This was done to allegedly free up beds, of which they estimated would amount to an extra 15,000 free beds within just one week of the directive being implemented.
It freed up so many beds that bed occupancy during April – June 2020 was 30% down on the previous year. Why on earth would these people already be in a hospital bed if they did not need to be? You attend hospital because you require medical treatment, not because you want a lie down and a good nights sleep.
This directive meant that people who required medical treatment and attention were discharged into Care homes in the thousands.
But Matt Hancock’s abandonment of the elderly and vulnerable didn’t end there. Whilst the NHS was busy discharging patients who required medical treatment into care homes under his directive, Matt Hancock and the Department of Health were busy trying to source them all a certain drug known as midazolam.

Midazolam is a commonly used drug in palliative care and is considered one of the four essential drugs needed for the promotion of quality care in dying patients in the United Kingdom. Think of it as diazepam on steroids.
Midazolam is also a drug that has been used in executions by lethal injection in the USA, combined with two other drugs. Midazolam acts as a sedative to make the prisoner unconscious. The other drugs then stop the lungs and heart working. However it has been the source of controversy as several prisoners took a long while to die and appeared to be in pain when midazolam was used.
Midazolam can also cause serious or life-threatening breathing problems such as shallow, slowed, or temporarily stopped breathing that may lead to permanent brain injury or death.
UK regulators state that you should only receive midazolam in a hospital or doctor’s office that has the equipment that is needed to monitor your heart and lungs and to provide life-saving medical treatment quickly if your breathing slows or stops.
A doctor or nurse should watch you closely after you receive this medication to make sure that you are breathing properly because midazolam induces significant depression of respiration. Your doctor should also be made aware if you have a severe infection or if you have or have ever had any lung, airway, or breathing problems or heart disease.
Midazolam is also used before medical procedures and surgery to cause drowsiness, relieve anxiety, and prevent any memory of the event. It is also sometimes given as part of the anesthesia during surgery to produce a loss of consciousness.
Midazolam is also used to cause a state of decreased consciousness in seriously ill people in intensive care units who are breathing with the help of a machine.
Midazolam should be used with extreme caution in patients who have chronic renal failure, impaired hepatic function, or impaired cardiac function. It should also be used with extreme caution in obese patients, or elderly patients.
What are some of the most important points you should take from this?
- Midazolam induces significant depression of respiration
- UK regulators insist midazolam should only be administered in a hospital or doctor’s office under the supervision of a doctor or nurse to monitor the breathing of the patient in order to provide life saving treatment to the patient if breathing slows or stops.
- Midazolam should be used with extreme caution in elderly patients
Serious illness in Covid-19 presents pneumonia and accompanying respiratory insufficiency. Therefore typical symptoms include breathlessness, cough, weakness and fever. We’re also told that people who suffer deteriorating respiratory failure and who do not receive intensive care, develop acute respiratory distress syndrome with severe breathlessness.
Midozalam induces significant depression of respiration.
Knowing that would you use midazolam to treat people who were suffering pneumonia and respiratory insufficiency allegedly due to Covid-19?
Well Matt Hancock and friends certainly seem to think so as you can see in the following video…
[embedded content]
The above exchange took place in a parliamentary committee meeting on the 17th April 2020 between Matt Hancock and Dr Evans, who is a fellow Conservative MP.
The following is an extract from an article which confirms the United Kingdom purchased two years worth of Midazolam in March 2020 and were looking to purchase much more –
Supplies of the sedative midazolam have been diverted from France as a “precaution” to mitigate potential shortages in the NHS caused by COVID-19, the Department of Health and Social Care (DHSC) has told The Pharmaceutical Journal.
A spokesperson from Accord Healthcare, one of five manufacturers of the drug, told The Pharmaceutical Journal that it had to gain regulatory approval to sell French-labelled supplies of midazolam injection to the NHS, after having already sold two years’ worth of stock to UK wholesalers “at the request of the NHS” in March 2020.
The DHSC said the request for extra stock was part of “national efforts to respond to the coronavirus outbreak”, which included precautions “to reduce the likelihood of future shortages”.
Why on earth would the United Kingdom need to purchase two years worth of Midazolam, a drug associated with respiratory suppression and respiratory arrest, to treat a disease that causes respiratory suppression and respiratory arrest?
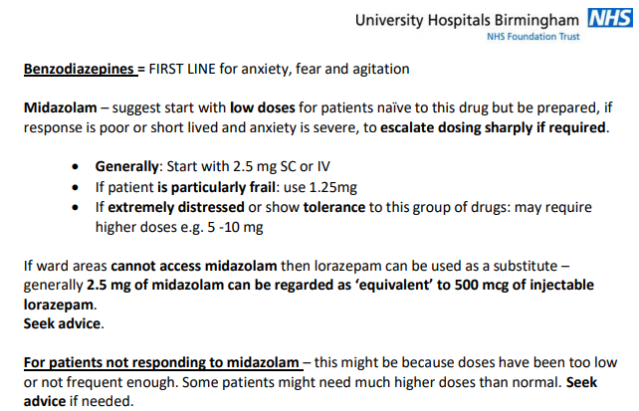
This document produced by the NHS states that Midazolam should be used for comfort at end of life care due to Covid-19 to ease fear, anxiety and agitation. Source

This NHS document states that midazolam should be used for sedation prior to the patient requiring mechanical ventilation, something we know has been required in hospitals for people who have developed severe pneumonia, of which we are told is due to Covid-19. However it also states that midazolam should only be used if 1st line and 2nd line drugs do not provide adequate sedation, but does include the caveat that midazolam alone can be added to 1st line drugs to reduce Propofol infusion rates. Source

This NHS document states that midazolam should be used for sedation prior to having a operation. Source

The same document also provides confirmation that midazolam has the potential to impair the respiration system, particularly in the presence of disease or old age. It clearly states that dosage should be kept to a minimum and shoud be within the manufacturer’s guidelines.

The document also provides a helpful table confirming dosage of midazolam for the elderly or unwell should be no more than 0.5mg – 1 mg, side effects include cardiorespiratory depression and the drug should be used with caution in those suffering respiratory disease.

This article confirms that over 2 million operations were cancelled at the end of March 2020 to free up beds for at least three months for “coronavirus” patients. – Source

Can you see the contradictions here? A policy that has been in place prior to the alleged emergence of Covid-19 clearly states that midazolam can be used for sedation, however dosage should be reduced to 0.5mg in the elderly or unwell due to possible side effects which include cardiorespiratory depression, and extreme caution should be used in administering midazolam to patients suffering respiratory disease.
However a policy created for treating patients allegedly suffering anxiety due to Covid-19, which we’re told is a respiratory disease, clearly states to treat said patient with a starting dose of 2.5mg of Midazolam, or 1.25mg if the patient is “particularly frail”, but to bump this up to 5 – 10mg if the patient is “extremely distressed”. Even the starting dose for the particularly frail is 0.25mg higher than the maximum recommended to administer to the elderly or unwell in sedation guidelines.
Who is responsible for making this decision and publishing these guidelines? And why is nobody holding them to account?
Two years worth of Midazolam was purchased in March 2020, however at the same time operations were cancelled for a minimum of three months, therefore Midazolam was not required for use in sedation prior to operations. Guidelines published prior to the alleged pandemic clearly state that Midazolam should be used in extremely low doses in the elderly or unwell, and should be used with extreme caution in those suffering respiratory disease due to side effects which include respiratory depression. We’re told Covid-19 is a respiratory disease and complications present pneumonia and severe respiratory distress. Therefore considering all of this the purchase of two years worth of Midazolam seems to be an awful waste of money, doesn’t it? As there doesn’t seem to be much they could possibly use it for within the guidelines
Well we can confirm it was definitely used as we have seen the prescription data.
But we’d just like to remind you of the important warning applied to Midazolam courtesy of the US National Library of Medicine –
Midazolam injection may cause serious or life-threatening breathing problems such as shallow, slowed, or temporarily stopped breathing that may lead to permanent brain injury or death. You should only receive this medication in a hospital or doctor’s office that has the equipment that is needed to monitor your heart and lungs and to provide life-saving medical treatment quickly if your breathing slows or stops. Your doctor or nurse will watch you closely after you receive this medication to make sure that you are breathing properly.
So can Matt Hancock explain why during April 2020 out of hospital prescribing for Midazolam was twice the amount seen in 2019?

According to official data in April 2019 up to 21,977 prescriptions for Midazolam were issued, containing 171,952 items, the vast majority being Midazolam Hydrochloride. However in April 2020 45,033 prescriptions for Midazolam were issued, containing 333,229 items, the vast majority being Midazolam Hydrochloride. That is a 104.91% increase in the number of prescriptions issued for Midazolam and a 93.85% increase in the number of items they contained. But these weren’t issued in hospitals, they were issued by GP practices which can only mean one thing, they were issued for end of life care.
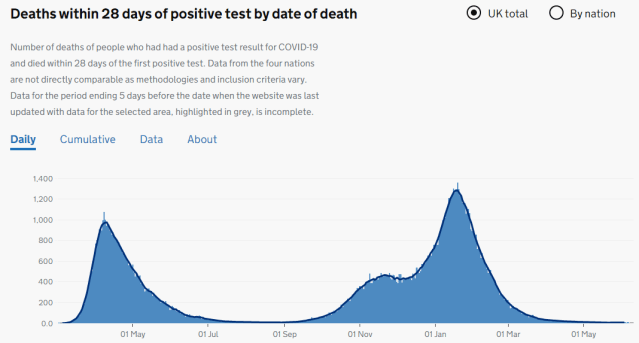
The above is a graph displayed on the UK Government website displaying deaths within 28 days of a positive test result for Covid-19 by date of death.
The following graph has been created using data on the amount of Midazolam solution produced each month from January 20219 through to March 2021.

Can you spot the difference? We couldn’t either because there isn’t one.
The spikes in production of Midazolam solution match the spikes of alleged Covid deaths within 28 days of a positive test.
April 2020 – huge surge in Midazolam prescriptions out of hospital and huge surge in production of Midazolam solution.
April 2020 – huge surge in alleged Covid deaths.
January 2021 – huge surge in production of Midazolam solution.
January 2021 – huge surge in alleged Covid deaths.
We’re told that serious illness in Covid-19 presents pneumonia and accompanying respiratory insufficiency. Therefore typical symptoms include breathlessness, cough, weakness and fever. We’re also told that people who suffer deteriorating respiratory failure and who do not receive intensive care, develop acute respiratory distress syndrome with severe breathlessness.
Midazolam Hydrochloride is associated with respiratory depression and respiratory arrest, especially when used for sedation in noncritical care settings. In some cases, where this was not recognized promptly and treated effectively, death or hypoxic encephalopathy has resulted. Intravenous midazolam hydrochloride should be used only in hospital or ambulatory care settings.
NHS policy prior to the emergence of Covid-19 states –
Dosage should be reduced to 0.5mg in the elderly or unwell due to possible side effects which include cardiorespiratory depression, and extreme caution should be used in administering midazolam to patients suffering respiratory disease.
NHS policy after the emergence of Covid-19, an alleged respiratory disease states –
Hospitals beds in April 2020 30% were down compared to the previous year.
A&E attendance was 57% down in April 2020 compared to the previous year.
Care home deaths were 205% up in April 2020 compared to April 2019.
The vast majority of alleged Covid deaths are people over the age of 85.
Can you not see a strong correlation here between the over prescribing of Midazolam and the seemingly premature ending of life, with the associated deaths being put down as Covid-19?
Did you really believe there’s a virus so clever that it knows to kill people who are disabled? Just look at the ONS statistics. Three in every five alleged Covid-19 deaths occurred in those who suffered learning difficulties and disabilities (see here).

In relation to deaths of people with learning difficulties the ONS said – ‘the largest effect was associated with living in a care home or other communal establishment.‘
Having a learning difficulty and being in care doesn’t mean you are more likely to die of Covid-19. What it means is that you are much more likely to have a DNR order placed on you without informing yourself or your family, which Carers / NHS staff then use as permission to put you on end of life care, which involves the administration of Midazolam.
We know this happened because an Amnesty report and CQC report said so.

The amnesty report states that –
‘Care home managers and staff and relatives of care home residents in different parts of the country told Amnesty International how, in their experience, sending residents to hospital was discouraged or outright refused by hospitals, ambulance teams, and GPs. A manager in Yorkshire said: “We were heavily discouraged from sending residents to hospital. We talked about it in meetings; we were all aware of this.”’
‘Another manager in Hampshire recalled:
There wasn’t much option to send people to hospital. We managed to send one patient to hospital because the nurse was very firm and insisted that the lady was too uncomfortable and we could not do any more to make her more comfortable but the hospital could. In hospital the lady tested COVID positive and was treated and survived and came back. She is 92 and in great shape.
She explained that:
There was a presumption that people in care homes would all die if they got COVID, which is wrong. It shows how little the government knows about the reality of care homes.‘

‘The son of one care home resident who passed away in Cumbria said that sending his father to hospital had not even been considered:
From day one, the care home was categoric it was probably COVID and he would die of it and he would not be taken to hospital. He only had a cough at that stage. He was only 76 and was in great shape physically. He loved to go out and it would not have been a problem for him to go to hospital. The care home called me and said he had symptoms, a bit of a cough and that doctor had assessed him over mobile phone and he would not be taken to hospital. Then I spoke to the GP later that day and said h would not be taken to hospital but would be given morphine if in pain. Later he collapsed on the floor in
the bathroom and the care home called the paramedic who established that he had no injury and put him back to bed and told the carers not to call them back for any Covid-related symptoms because they would not return. He died a week later.
He was never tested. No doctor ever came to the care home. The GP assessed him over the phone. In an identical situation for someone living at home instead of in a care home, the advice was “go to hospital”. The death certificate says pneumonia and COVID, but pneumonia was never mentioned to us.’
‘A care home manager in Yorkshire told Amnesty International:
In March, I tried to get [a resident] into hospital—the ambulance had employed a doctor to do triage but they said, “Well he’s end of life anyway so we’re not going to send an ambulance” … Under normal circumstances he would have gone to hospital … I think he was entitled to be admitted to hospital. These are individuals who have contributed to society all their lives and were denied the respect and dignity that you would give to a 42-year-old; they were [considered] expendable.‘
The CQC felt it necessary to issue a statement in August 2020 addressing the issue of innapropriate DNR’s being placed on care home residents without informing the resident or their family –
‘It is vitally important that older and disabled people living in care homes and in the community can access hospital care and treatment for COVID-19 and other conditions when they need it during the pandemic … Providers should always work to prevent avoidable harm or death for all those they care for. Protocols, guidelines and triage systems should be based on equality of access to care and treatment. If they are based on assumptions that some groups are less entitled to care and treatment than others, this would be discriminatory. It would also potentially breach human rights, including the
right to life, even if there were concerns that hospital or critical care capacity may be reached.’
That statement was issued because the CQC found that 34% of people working in health and social care were pressured into placing ‘do not attempt cardiopulmonary resuscitation’ (DNACPR) orders on Covid patients who suffered from disabilities and learning difficulties, without involving the patient or their families in the decision.
The evidence is all there to see in the public domain and thankfully, a team of people are gathering said evidence and analysing it, so that justice can be sought for the people that have had their lives ended prematurely via the use of inappropriate DNR orders, used as permission to start end of life treatment which included a drug called Midazolam. A drug that is associated with respiratory depression and respiratory arrest, the exact same symptoms of complications due to the alleged Covid-19 disease, especially when used for sedation in noncritical care settings.
A drug which was ordered by UK authorities in March 2020 at a quantity to cover a usual two year supply. A two year supply that seems to have been depleted by October 2020 according to NHS documents –
But once replenished the stocks were again depleted by the beginning of February 2021 according to official NHS documents –
It was decided in 2013 after a review that the ‘Liverpool Care Pathway‘ was to be abolished. The Liverpool Care Pathway (LCP) was a scheme that we’re told intended to improve the quality of care in the final hours or days of a patient’s life. It’s alleged aim was to ensure a peaceful and comfortable death. The LCP was a guide to doctors, nurses and other health workers looking after someone who was dying on issues such as the appropriate time to remove tubes providing food and fluid, or when to stop medication.
The reason it was decided it should be abolished is that the review found hospital staff wrongly interpreted its guidance for care of the dying, leading to stories of patients who were drugged and deprived of fluids in their last weeks of life.
The government-commissioned review, headed by Lady Neuberger, found that poor training and a lack of compassion on the part of nursing staff was to blame. Harrowing stories from families revealed they had not been told their loved one was expected to die and, in some cases, were shouted at by nurses for attempting to give them a drink of water. Nursing staff had wrongly thought, under the LCP guidance, that giving fluids was wrong.
The review made 44 recommendations, including the phasing out of the LCP over six to twelve months as individual care plans for the dying were brought in. It stated that only senior clinicians must make the decision to give end-of-life care, along with the healthcare team, and that no decision must be taken out of hours unless there is a very good reason.
The evidence suggests that the Liverpool Care Pathway returned with a vengeance in April 2020 under the direction of the Health Secretary Matt Hancock, Government Advisors and NHS Chiefs, and it looks as if it was used to manipulate you into giving up over one year of your life under the pretence that you were staying at home, to protect the NHS and save lives. But the evidence suggests that in reality you were ordered to stay at home, to protect the NHS, so that they could prematurely end the lives of the elderly and vulnerable and tell you that they were Covid deaths.
Midazolam. It should be the word that is on everyone’s lips. We’re sure it will be now.


