Religiosity and beliefs in medical conspiracy theories in 37 European countries during the COVID-19 pandemic
Abstract
While beliefs in conspiracy theories related to medical procedures proliferated in Europe during the COVID-19 pandemic, previous research has focussed on such predictors of conspiracy as age, gender, educational status, political orientation, and trust in science. By analysing the data from the Eurobarometer survey conducted in 2021 in 37 European countries, this study describes the association between beliefs in medical conspiracy theories and religiosity. It reports three significant findings: first, medical conspiracy theories are more prevalent in the Baltic, Balkan, Southern, Central, and Eastern European countries; second, people who declare themselves to be religious are more willing to believe in medical conspiracy theories; and third, Muslims, Catholics, and Orthodox Christians demonstrated stronger support for medical conspiracy theories than other faith groups and non-believers. Analysing data at both the individual and country level sheds light on the role of religion as a predictor of a conspiracy belief, which may influence people’s medical and health behaviours.
Similar content being viewed by others

Introduction
Today’s Western world is often described as a ‘post-truth’ culture in which opinions are not based on objective (i.e., scientific) facts but formed by emotional appeal (Lewandowsky et al., 2017; Lockie, 2017; Malcolm, 2021; Speed & Mannion, 2017). The ‘post-truth’ society has emerged as a consequence of a ‘fluid’ modern world manifested by social mega-trends, such as globalisation, the decline in social capital, increased social polarisation and economic inequalities, and the expansion and fragmentation of the media landscape. It is characterised by uncertainty, privatisation, ambivalence, and the constant ‘production’ of new truths, norms, and values (Bauman, 2000).
While the terms ‘post-truth’ or ‘post-fact’ are associated with the declining trust in scientific knowledge and the transformation of political culture, they refer to circumstances in which personal beliefs and emotions become more influential in forming public opinion than objective facts, which, in turn, makes it difficult to distinguish the real from the false (Lockie, 2017; Malcolm, 2021). Thus, while the post-truth era represents the triumph of subjective feelings, emotions, and psychological factors over objective evidence and facts, it also refers to the relativisation of truth, the manipulation of knowledge, and the polarisation of views, which fuel conspiracy theories (Harambam et al., 2022).
Conspiracy theories are usually defined as narratives that assume the existence of small but powerful groups of people or organisations acting in secret to achieve some, typically sinister, purpose against the common good (Uscinski & Enders, 2023; van Prooijen & Douglas, 2017). Although numerous conspiracy theories have emerged in the public discourse in recent decades, including those related to the flat-Earth theory, the moon landings, Area 51 and alien technology, John F. Kennedy’s assassination, GMOs, or 9/11 (van Prooijen, 2018; Uscinski, 2018), less attention has been paid to medical-focused conspiracy theories.
However, although suspicions regarding medical procedures are currently on the rise, such suspicions have always existed (Andrade, 2020; Blaskiewicz, 2013; Marques et al., 2022; Nattrass, 2023). Moreover, since medical conspiracy theories or health-related conspiracies encompass a wide range of themes, they are widely believed in many societies (Lahrach & Furnham, 2017; Marques et al., 2022; McCarthy, 2014; Oliver & Wood, 2014a). At the same time, although medical conspiracy theories vary widely, some are more popular than others. Arguably, the most widespread and commonly believed medical conspiracy theories refer to vaccination. Nonetheless, opposition to vaccination dates to its introduction in the early 19th century, when the cowpox vaccination invented by Edward Jenner provoked sanitary, religious, scientific, and political objections (Andrade, 2020; Wolfe & Sharp, 2002). It also flourished in 1998, when Dr Andrew Wakefield and his colleagues published a paper in The Lancet suggesting that the measles, mumps, and rubella (MMR) vaccine causes autism (Davidson, 2017; Wakefield et al., 1998). Furthermore, numerous anti-vaccination theories spread rapidly across many countries during the COVID-19 outbreak, suggesting that mRNA vaccines modify the human genome, contain microchips to control people, or were designed to cause infertility and depopulate societies (Pertwee et al., 2022; Shahsavari et al., 2020; Uscinski, Enders, Klofstad et al., 2022).
Other popular medical conspiracy theories include human immunodeficiency virus (HIV) denialism (Duesberg, 1992; Kalichman et al., 2010) and that numerous viruses, including HIV, Zika, Ebola, MERS, and SARS-CoV, have been designed and manufactured as bioweapons (Geissler & Sprinkle, 2013; Imhoff & Lamberty, 2020). Besides, some medical conspiracy theories argue that water fluoridation and dental fluorosis cause numerous diseases, including cancer and Alzheimer’s (Armfield, 2007; Carstairs, 2015), or that remedies for most human diseases are already known but are hidden by Big Pharma and ‘the scientific establishment’ so they can earn more from modern medications (Andrade, 2020; Blaskiewicz, 2013; Oliver & Wood, 2014a).
Beliefs in medical conspiracy theories have important implications for public health since people’s support for medical conspiracy theories influences their medical and health behaviours. Some studies suggest that while searching for health information, people who believe in medical conspiracy theories are less likely to rely on conventional medicine and family physicians; instead, such individuals turn to the Internet as well as alternative and complementary medicine (Fournier & Varet, 2023; Ladini, 2022; Oliver & Wood, 2014a; Soveri et al., 2021). They are also more likely to endorse mythical causes of cancer and avoid cancer screening (Sonia et al., 2022). Finally, during the COVID-19 pandemic/infodemic, people who supported conspiracy theories were less likely to follow a prescription regimen (using face masks, sanitisers, and social distancing) or to be tested for and vaccinated against COVID-19 (Jabkowski et al., 2023; Kwok et al., 2023; Łowicki et al., 2022; Marques et al., 2022; Nally, 2022; Nattrass, 2023; Parmet & Paul, 2020; Walkowiak et al., 2022).
While several factors influencing a conspiracy belief have been identified, including gender, age, and various personality traits, numerous studies have shown that people’s beliefs in conspiracy theories are strongly associated with educational status, political orientation, and trust in science (Douglas et al., 2016; Frenken et al., 2023; Roozenbeek et al., 2020; Soveri et al., 2021; Uscinski, Enders, Diekman, et al., 2022). At the same time, much less attention has been directed at studying the relationship between religion/religiosity and beliefs in medical conspiracy theories. Some research has, however, demonstrated that religious people are more suspicious of science and have lower levels of science literacy (Heidi Oi-Yee et al., 2020; McPhetres & Zuckerman, 2018). For example, some recent studies have revealed an association between spirituality and personal religiosity and human papillomavirus (HPV) vaccine hesitancy and higher support for conspiracy theories related to the coronavirus and COVID-19 vaccinations (Jabkowski et al., 2023; Kosarkova et al., 2021; Łowicki et al., 2022; Pavić & Šuljok, 2022; Tonković et al., 2021). At the same time, it is often argued that it is not religion itself that fuels beliefs in conspiracy theories but rather religious fundamentalism (Yendell & Herbert, 2022). For example, while Beller (2017) found strong association between religious conspiracy belief, religious fundamentalism and militarism, both Łowicki et al. (2022) and Sobol et al. (2022) demonstrated that since religious fundamentalism, unlike centrality of religiosity, was positively related to coronavirus conspiracy beliefs, people who were religious fundamentalists held more conspiracy theories and were less likely to follow public health guidelines about the COVID-19 epidemic.
To fill this empirical gap, we aim to explore the association between religiosity and beliefs in medical conspiracy theories, including (1) the association between declared religiosity, professed religion, and individual beliefs in medical conspiracy theories and (2) cross-country differences in religiosity and support for medical conspiracy theories in Europe.
Methods
Study design and data sources
All analyses in this paper utilise data from the Eurobarometer survey (EB edition 95.2; 2021) commissioned by the Directorate-General Communication of the European Commission and the European Parliament. The survey was carried out between 13 April and 11 May 2021 by the Kantar network and conducted in all 27 European Union Member States as well as five candidate countries (Albania, Montenegro, North Macedonia, Serbia, and Turkey) and Bosnia and Herzegovina, Iceland, Norway, Switzerland, and the United Kingdom.
The primary sample design applied in most countries was a multi-stage stratified random probability sampling of individuals taken from a population of residents aged 15 years and over in each country; however, a mix of probability and nonprobability designs was implemented in some countries. As the fieldwork was carried out during the COVID-19 pandemic, interviews were conducted through face-to-face computer-assisted personal interviews and self-administered computer-assisted web interviews. Of the 37 countries listed above, computer-assisted personal interviews were implemented in 17, where interviews were conducted outside respondents’ homes to remain in the open air and maintain social distancing between the interviewer and respondent. In turn, mixed modes, namely, both face-to-face and online interviewing, were observed in six countries, while in the remaining 14 (where personal interviewing was not possible under COVID-19 restrictions), interviews were conducted purely online (the overall sample size for all countries equals 36,025 respondents).
Table A1 in section 2.1 of the supplementary online appendix lists countries with modes of data collection and response rates. Besides, Table A1 presents descriptive statistics for the outcome variable (i.e., beliefs in medical conspiracy theories; see the operationalisation below) and for the three characteristics (at the country level) that we used to demonstrate the correlation between aggregated individuals’ beliefs in medical conspiracy theories and the (a) country-level fraction of ‘very religious’ citizens, (b) the dominant religion, and (c) the Herfindahl–Hirschman Index measuring the concentration of professed religions in each country (for the specifications of these variables, see subsection ‘Country-level contextual data’).
Ethical issues
This study exclusively used publicly available anonymised data; hence, no ethics approval was required. All data are publicly available via the GESIS Leibnitz Institute for the Social Sciences website (European Commission, 2022).
Outcome variable
Beliefs in medical conspiracy theories constitute the dependent variable in our analysis. Respondents were presented with statements about the natural and physical sciences, medicine, natural history, demography, and geography and asked whether they believed them to be true or false. Two of the 11 statements were directly connected with medical conspiracy theories and intentionally false, namely, (a) ‘the cure for cancer exists but is hidden from the public by commercial interests’, and (b) ‘viruses have been produced in government laboratories to control our freedom’. If respondents indicated ‘true’ for at least one of the above items, we classified them as believers in medical conspiracy theories. Thus, the dependent variable is dichotomous: respondents who agreed with at least one statement were assigned code 1 and the rest code 0.
Covariates
According to the theoretical assumptions, we included two variables to explain why respondents vary in their belief in medical conspiracy theories: their religiosity and professed religion. Religiosity was measured by asking respondents to consider how religious or spiritual they are on a 10-point scale ranging from 1 (not at all religious or spiritual) to 10 (very strongly religious or spiritual). In turn, respondents’ professed religion was obtained from the survey participants’ questions about whether they considered themselves non-believers, atheists, agnostics, or believers of one of several religions. We assigned each respondent to one of six empirical categories: [1] Atheists or agnostics (including non-believers), [2] Catholics, [3] Orthodox Christians, [4] Protestants and other Christians, [5] Muslims (including Shia, Sunni, and other Muslims), and a group of [6] ‘Others’, covering adherents to religions that rarely appeared in a sample (i.e., Jews, Sikhs, Buddhists, and Hindus; the size of each group within each country was too small to make any valuable generalisations).
Control variables
Our analysis incorporated four control variables at the respondent level: gender, age, educational level, and trust in scientists. Gender was indicated as 1 (woman) and 0 (man), while age was expressed in the number of years and standardised across all countries and respondents before being included in the regression analysis (zero means the average year of the respondents in the EB data). In turn, the level of education was established by asking respondents about the highest level of education they had completed (Eurobarometer assigned respondents to 20 different categories with increasing levels of education; note that we standardised the educational level across the whole sample; consequently, zero indicates the average educational category across all respondents included in the EB).
Finally, trust in scientists was measured as a latent construct based on three items asking respondents to assess the extent to which they agreed with the following statements regarding scientists today: [1] ‘we can no longer trust scientists to tell the truth about controversial scientific and technological issues because they depend increasingly on money from industry’, [2] ‘scientists only look at very specific issues and do not consider problems from a wider perspective’, and [3] ‘nowadays, the problems we are facing are so complex that scientists are no longer able to understand them.’ The response options were set up as follows: Totally agree (score 1), Tend to agree (score 2), Neither agree nor disagree (score 3), Tend to disagree (score 4), and Totally disagree (score 5). We calculated the overall score of the scale ‘trust in scientists’ (the higher the score, the higher the trust) as a sum of scores on three items and standardised the sum across all countries and respondents (so that zero corresponds to the average score of trust for all respondents included in the EB) before including the variable in the regression analysis (note that the standardised Cronbach’s alpha for such a scale equals 0.73, suggesting its good internal consistency, while multigroup confirmatory factor analysis allows us to assume the scale fulfils the assumption of configural and metric cross-country invariance, which are necessary conditions to ensure the equivalence of the meaning of regression coefficients in different countries; for details of how the constructed scale was evaluated, consult supplementary online appendix, Table A2 and A3 in section 2.2.).
Country-level contextual data
Motivated by the fact that the respondents formulated their opinions and beliefs through the prisms of the different sociocultural and religious contexts in which they were socialised and in which they lived (e.g., Finke & Adamczyk, 2008; Müller et al., 2014; Ruiter & De Graaf, 2006; Ruiter & Van Tubergen, 2009), we also included three contextual variables to check whether (a) the overall country-level fraction of ‘very’ religious respondents, (b) the dominant religion in a given country, and (c) the concentration of professed religions within each country could explain cross-country differences in the overall fraction of respondents that believed in medical conspiracy theories. We derived all three contextual characteristics directly from the Eurobarometer data by manipulating the marginal distributions on two explanatory variables introduced previously in the subsection ‘Covariates’. Firstly, the overall country-level fraction of ‘very’ religious respondents represents the country-share of respondents that indicated at least a score of 7 on a 10-point scale of religiosity or spirituality. Secondly, a country’s dominant religion indicates the most popular answer on professed religion. Finally, as a dominant religion does not take into account the distribution of the professed religion and only considers which is the most popular, we calculated the Herfindahl–Hirschman Index, measuring the concentration of professed religions in each country; note that the Index varies from 0 (perfect diversity of different professed religions, i.e., uniform distribution) to 1 (concentration of only one religion).
Analytical approach
In order to recognise the hierarchical structure of Eurobarometer data (with respondents nested within countries) and test the impact of the respondents’ religiosity and professed religion on their beliefs in medical conspiracy theories (dichotomous outcome) while controlling sociodemographic characteristics and trust in scientists at the individual level as well as of contextual data at the country-level (i.e., a fraction of ‘very’ religious respondents, the dominant religion, and concentration of professed religions), we implemented a series of multilevel regression models (assuming random intercepts between countries in each model) with all variables added to the regressions in a stepwise manner:
-
We started with the null model (which excludes all variables from the regression), allowing us to estimate the variance components (i.e., intraclass correlation coefficient) attributed to the country level.
-
Model 1.1 added the fraction of ‘very’ religious respondents as a country-level contextual variable.
-
Model 1.2 added the dominant religion as a country-level contextual variable.
-
Model 1.3 added the concentration of professed religions as a country-level contextual variable.
In the models (1.1–1.3), we introduced country-level contextual variables individually instead of incorporating them into a single regression. This decision was motivated by the relatively small number of countries in our comparison, which raised the potential for overfitting the model and limited the statistical power of analysis, that is, the ability to identify significant effects. Models 1.1–1.3 allowed us to estimate the relative decrease of the intraclass correlation coefficient compared to the null model and check which contextual variables best explained between-country differences in the overall fraction of respondents that believe in medical conspiracy theories.
In addition, we ran two models (2.1 and 3.1) to assess whether respondents’ beliefs in medical conspiracy theories depended on their religiosity and professed religion, respectively (two separate bivariate models, each with only one predictor), as well as two ‘fully-adjusted’ models (2.2 and 3.2) that checked whether respondents’ gender, age, educational level, and trust in scientists did not make relationships from bivariate models negligible (Model 2.2. adjusted religiosity and Model 3.2. professed religion). In every model, we also checked whether the relationship between religiosity and professed religion was constant across countries, allowing regression slopes to vary. Moreover, we separately estimated models for two explanatory variables, as the random slope cross-country model with both covariates in one model could introduce the problem of collinearity and the risk of loss of precision when we compared (only) 37 countries. In all analyses, population size weights were incorporated, with each national sample being adjusted in proportion to its share in the total population aged 15 and over across all countries. Additionally, post-stratification weighting factors were included. The supplementary online appendix (sections 1.3 and 1.4) contains the detailed technical specifications of the regression models. We conducted all analyses in the R Project for Statistical Computing (R Core Team, 2023) with the packages for data analyses and visualisation listed in an online appendix.
Results
We started with descriptive results comparing the average country-level fraction of respondents believing in medical conspiracy theories across 37 European countries. Then, we moved to regression analysis to examine whether country-level contextual variables allowed us to explain differences observed between European countries in an outcome variable. Finally, we tested whether religiosity and professed religion, at the individual level, significantly correlated with the propensity to believe in medical conspiracy theories, and we also checked how these effects vary in European countries.
Descriptive results: beliefs in medical conspiracy theories across Europe
Figure 1 displays a map of Europe that visualises notable between-country differences in the fraction of respondents who believed in medical conspiracy theories (the average fraction for all 37 countries equals 0.606). The group of ‘red’ countries, namely, those where the country-level fraction is above the average, is constituted mainly by all the Balkan states, Southern Eastern countries, Central and Eastern European countries (apart from Czechia, significantly below average), and the Baltic states (except for Estonia, slightly below average). In turn, a group of ‘green’ countries (where the fraction of respondents that believed in medical conspiracy theories is below the average for all countries covered by the Eurobarometer 95.2 survey) is formed by all the Scandinavian countries, Finland, three Benelux states, the UK, Ireland, and Western European countries (including Austria, Germany, France, and Switzerland). Finally, the level of belief in medical conspiracy theories in Southern countries, including Italy, Portugal, and Spain, was around the average value.
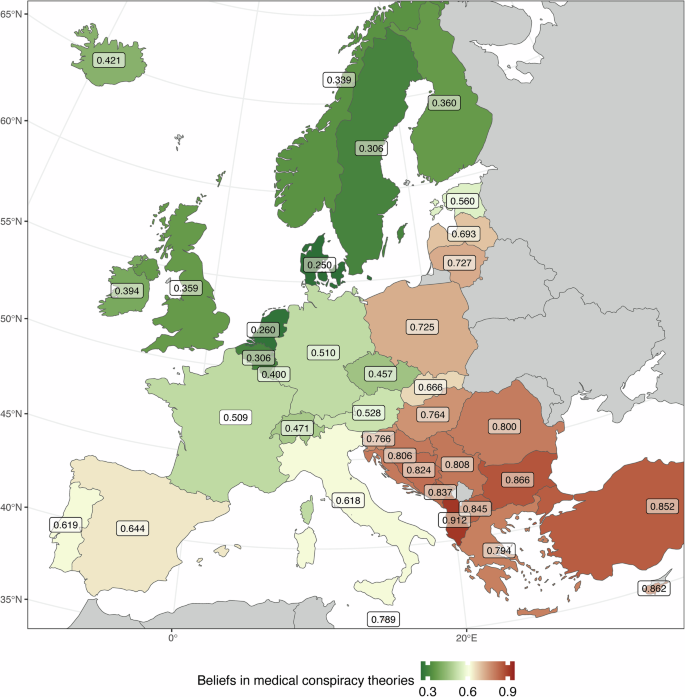
Beliefs in medical conspiracy theories across European countries.
In the next step of the analysis, we demonstrated that the variation in the fraction of respondents that believed in medical conspiracy theories in European countries can be attributed to the differences in the contextual variables, that is, the country-level percentage of ‘very’ religious respondents, the dominant religion, and the concentration of the professed religions in a country.
Regression results: religiosity and professed religion shape beliefs in medical conspiracy theories at country and individual levels
Table 1 summarises the results of the multilevel regression null model (with respondents nested within 37 countries) and three models (1.1–1.3) with country-level predictors added to explain variation in beliefs in medical conspiracy theories across European countries. The intraclass correlation coefficient (ICC) value in the null model indicates that 18.5 per cent of the total variation in the respondents’ beliefs in medical conspiracy theories can be attributed to the differences between countries; thus, as the ICC exceeds the cut-off value of 5 per cent (Heck, Thomas & Tabata, 2013, p. 8), the multilevel approach is justified. Note that by including all three country-level contextual variables, namely, the fraction of ‘very’ religious citizens, the dominant religion, and the concentration of professed religion, we significantly reduced the unexplained cross-country variance to 8.8, 4.0 and 10.9 per cent, respectively. The latter means that, among two others, the dominant religion in a country has the best predictive power to explain why countries differ. Nevertheless, the regression coefficients for all three country-level predictors are significant, and the relationships are in the direction we expected. More importantly, the results confirmed that the respondents formulated their beliefs about medical conspiracy theories through the prism of the country contexts in which they were socialised and where they lived. We demonstrated that these contexts refer directly to the issue of religion and religiosity.
To facilitate the interpretation of country-level associations indicated by regression models 1.1–1.3, we plotted them in Fig. 2. Each dot represents one country (identified by country codes). The country’s position was determined by the average fraction of respondents who believed in medical conspiracy theories (on the x-axis) and the overall fraction of ‘very’ religious respondents (on the y-axis). In contrast, the colour of the dots represents the dominant religion in a country, and the size of the dots corresponds to the concentration of the dominant religion. In addition, the dashed line represents the linear relationship between the x-axis and y-axis (with a grey area corresponding to the 95% confidence interval of the linear model of the relationship), with Pearson’s linear correlation coefficient and its significance level presented in the left upper corner of the plot.
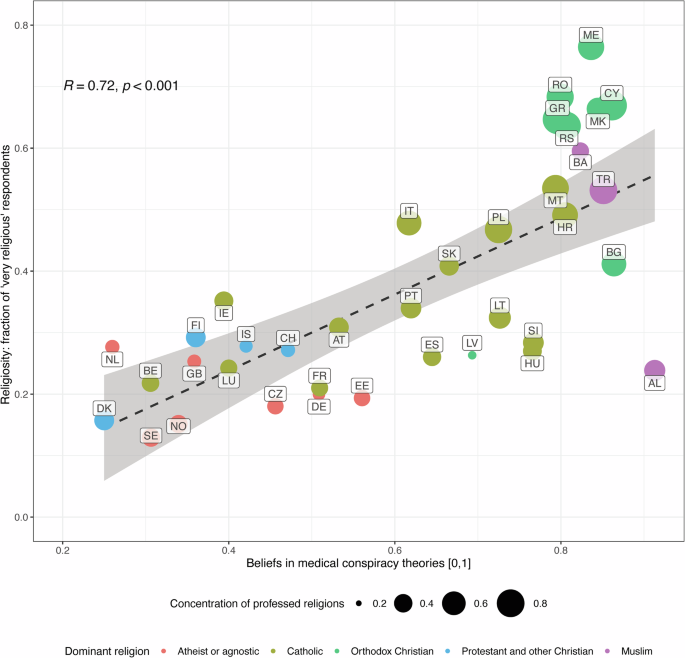
Country-level associations between beliefs in medical conspiracy theories and contextual variables.
Figure 2 indicates that the higher the country-level fraction of ‘very’ religious citizens, the more people believe in medical conspiracy theories; a similar positive relationship exists for the concentration of professed religions. In turn, for the dominant religion, we observed that (compared to countries where atheists and agnostics are in the majority), the highest support for medical conspiracy theories was in countries where Muslims were the dominant group. The level of support was generally also significantly higher in groups of countries where Orthodox Christians and Catholics dominated, while in countries where Protestants and other Christians constituted the dominant group, the fraction of respondents supporting medical conspiracy theories was on a similar average level to that in the countries dominated by atheists and agnostics (with no significant differences between the two groups of countries). The results, therefore, show strong geographical patterns of support for medical conspiracy theories. Such support was lower in Western European and Scandinavian countries (historically dominated by Protestantism) and had much greater religious diversity. It was higher in Central and Eastern European countries, Southern Europe, the Balkans and Turkey, where Catholicism, Orthodox Christianity, or Islam dominate and religious diversity is lower. On the other hand, support for medical conspiracy theories was also strongly related to the country-level fraction of ‘very’ religious respondents, which, in turn, may be partly the result of different patterns of religiosity that characterise a particular religion or denomination. Thus, all three country-level contextual variables related to the issue of religion may overlap but still play a central role in shaping attitudes towards medical conspiracy theories.
Our final analyses worked on respondent-level data and aimed to investigate whether an individual’s religiosity and professed religion significantly impact their propensity to believe in medical conspiracy theories. Table 2 summarises bivariate (Models 2.1 and 3.1) and fully adjusted multilevel regressions (Models 2.2 and 3.2) specified in the subsection presenting our analytical approach.
The multilevel regressions (with individual-level covariates) confirmed the supposition that religiosity significantly increases the odds of supporting medical conspiracy theories (Model 2.1) and that the relationship stands even when adjusting for gender, age, educational level, and trust in scientists (Model 2.2). Note that we also tested whether country-level variables moderate the association between religiosity and the outcome variable and found that the concentration of professed religions strengthens the effect of religiosity (for details see online supplementary appendix section 1.5.). Similarly, we confirmed that the religion professed by respondents significantly impacted the odds of their believing in medical conspiracy theories, both in a bivariate Model 3.1 and fully adjusted Model 3.2. Note that compared to the atheist and agnostic respondents, respondents defining themselves as Catholics, Orthodox, Protestants, Muslims, or believers of any other religion had a significantly higher odds ratio of also believing in medical conspiracy theories. For example, when the respondents declared themselves to be Muslims, their odds of believing in medical conspiracy theories were almost 4.5 times higher (in a bivariate model) and nearly three times higher (in a fully adjusted model) than those of their atheist and agnostic counterparts. Thus, at both the country and respondents’ levels, professed religion and religiosity correlated with belief in medical conspiracy theories.
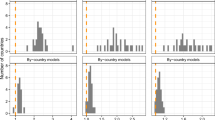
In all the models presented in Table 2, we allowed for the associations between two explanatory variables, religiosity and professed religion, and the outcome variable, belief in medical conspiracy theories, to vary between countries. We did so to test whether the impact of religiosity and professed religion was constant in all the European countries under investigation; if it was, the result would strengthen the generality of our conclusions. As Table 2 presents the marginal effects of the relationships (i.e., the aggregated results of the associations observed in every country), not the between-country differences in the strength and direction of the relationship, we additionally demonstrate, in Fig. 3, the density curves and histograms of the distribution odds ratios for religiosity and professed religion derived (for each country) from the bivariate (left panels) and fully adjusted (right panels) regression models. The vertical dashed line was set up at an odds ratio equal to 1.0 and indicates no effect of the explanatory variable; the values above 1 indicate countries where the variable enhanced (and the values below 1 imply the countries where the variable weakens) the probability that respondents would believe in medical conspiracy theories. Consult the supplementary online appendix section 2.3. for the exact values of odds ratios for both explanatory variables obtained in every country from the bivariate (Table A4) and fully adjusted models (Table A5).
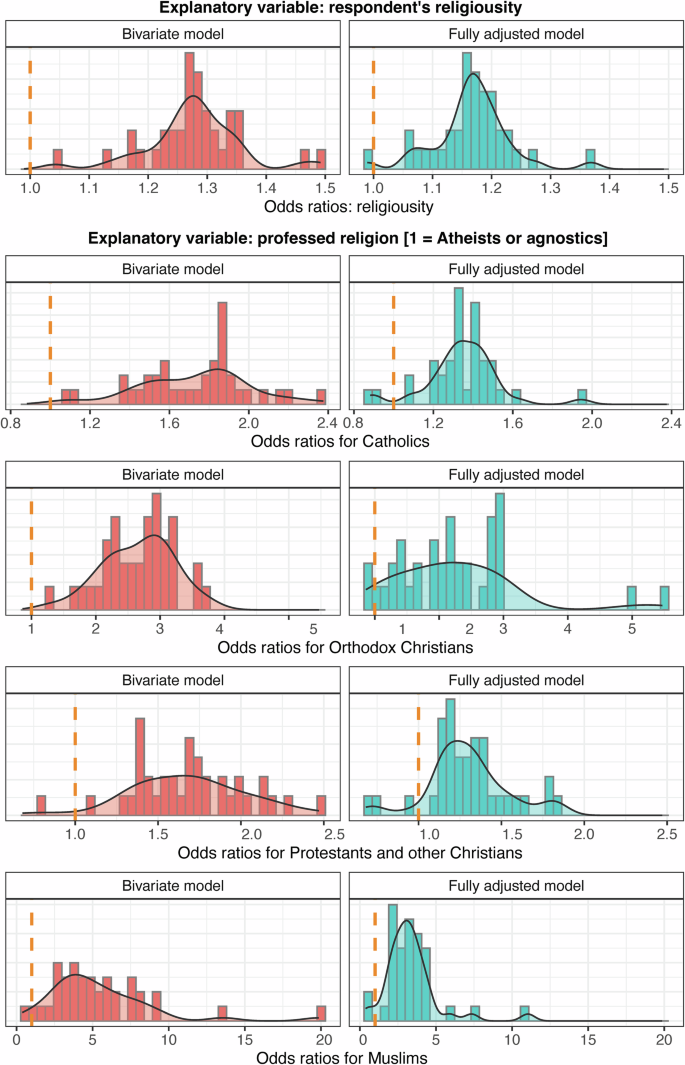
Density curves and histograms of the distribution odds ratios for religiosity and professed religion derived from the bivariate and fully adjusted regression models.
As demonstrated in Fig. 3, the direction of the impact of religiosity and professed religion on the odds ratios of belief in medical conspiracy theories observed for every country in the bivariate and fully adjusted models aligns with the general associations indicated in Table 2, with only a few exceptions. For example, when analysing the distribution of the odds ratios for religiosity for all 37 countries, the parameters were estimated at the value above 1 in a bivariate analysis, while in a fully adjusted model, the regression parameters were above the reference value of 1.0 except for Germany (where the value was slightly below). Similarly, compared to the atheists and agnostics (constituting the reference category for the believers of other religions), the odds ratios in the bivariate and fully adjusted models for Catholics, Orthodox Christians, Protestants and other Christians, Muslims, and respondents who professed different religions were higher in almost every country. The only exceptions to this general rule were in fully adjusted models: Germany (for Catholics and Protestants), Spain (for Catholics and Orthodox Christians), the United Kingdom (for Protestants), Poland (for Muslims), Sweden (for Orthodox Christians), and Turkey (for Protestants and Muslims). However, note that the observed distributions of odds ratios (even if some exceptions exist) are less likely under the assumption of no assumed directions of the relationship between beliefs in medical conspiracy theories and individuals’ religiosity and professed religion, demonstrating that the relationship pattern is almost universal across Europe.
Discussion
This article reports three significant findings. First, while it shows that medical conspiracy theories are spread across Europe, they are more prevalent in the Baltic, Balkan, Southern, Central, and Eastern European countries than in Scandinavian and Western European ones. However, this finding should not be surprising since previous studies also revealed a significant cross-country variation between Northern and Western Europe and Central and Eastern Europe and the Balkan states, as the latter had higher levels of belief in conspiracy theories (Drochon, 2018; Imhoff et al., 2022; Jabkowski et al., 2023).
Second, and more importantly, researchers often focus on such predictors of conspiracy as age, gender, educational status, political orientation, and trust in science (Douglas et al., 2016; Frenken et al., 2023; Roozenbeek et al., 2020; Soveri et al., 2021; Uscinski, Enders, Diekman, et al., 2022), our analysis demonstrated that people who declare themselves to be religious are more willing to believe in medical conspiracy theories than non-believers (i.e., atheists and agnostics). In other words, we showed that religiosity is a significant predictor of support for medical conspiracy theories (cf. Frenken et al., 2023). Thus, our findings shed light on the complex and often not obvious relationship between religiosity and beliefs in medical conspiracy theories across 37 European countries (Douglas et al., 2019; Ladini, 2022; Łowicki et al., 2022). By examining the ‘post-truth’ culture’s influence on healthcare perceptions and considering the association of subjective beliefs on public health behaviour, this research contributes to understanding the nuanced dynamics of how religiosity intertwines with medical conspiracy theory endorsement. The emergence of a ‘post-truth’ culture in the Western World has marked a shift whereby subjective emotions and beliefs often outweigh objective facts and scientific evidence (Compton et al., 2021). The results align with previous research showing a pervasive impact of conspiracy theories, especially in the medical domain (Andrade, 2020; Imhoff & Lamberty, 2020; Oliver & Wood, 2014a, 2014b). The prevalence of medical conspiracy theories, encompassing notions such as vaccination scepticism, hidden cures for diseases, and suspicions regarding pandemic responses, presents a formidable challenge in public health advocacy and intervention strategies (Douglas et al., 2015).
Third, while our investigation underscores the correlation between higher levels of religiosity and beliefs in medical conspiracy theories, it also demonstrates that believers of some confessions are more prone to believe in conspiracy theories (Mashuri & Osteen, 2023; Nefes & Aksoy, 2024). Notably, individuals identifying as Muslims demonstrate a strong association with beliefs in medical conspiracy theories, followed by Catholics and Orthodox Christians. However, the impact varies across countries, suggesting a complex interplay between religiosity and cultural contexts in shaping medical conspiracy theory endorsement. Other studies have also shown that followers of particular religions are more sceptical regarding science and medical knowledge than others. For example, Muslims and Orthodox Christians have the lowest levels of optimism when it comes to generalised technological optimism (EB, 2010, pp. 89–90) and have the most ethical objections to human embryonic stem cell research (EB, 2010, pp. 90–91).
Thus, while no religion seems immune to conspiracy theories, this study shows that some denominations are particularly susceptible. In fact, it was suggested that especially religions that adhere to traditionalism, conservatism, and fundamentalism and are convinced that they alone hold absolute truth and that religion does not have enough influence on politics are more conducive to conspiracy theories (Beller 2017; Yendell, & Herbert, 2022). Moreover, Robertson and Dyrendal (2018) suggest that conspiracy theories and religions share some common concepts such as prophecy, revaluation, millennialism or apocalypticism, esotericism, and the paranormal, which become a source of “grand explanatory narratives” disclosing mysteries, provide meaning and rationalisations or explanations of unusual or morally puzzling events frequently leading to general mistrust towards social institutions. Thus, since many conspiracy beliefs have many quasi‐religious elements, refer to and are fuelled by paranormal and apocalyptic beliefs (Frenken et al., 2023), i.e. QAnon conspiracy theory, they may be particularly attractive to followers of those religions where such elements are also present. For example, Beyer and Herrberg (2023) demonstrated that due to its biblicism, the conviction that its understanding of reality contains absolute truth (nomization), that good and evil can be distinguished with clarity (Manichaeism), and that political action can bring about salvation (immanent eschatology) evangelicalism attracts more persons who hold conspiracy beliefs. Similarly, recent studies conducted in Poland showed that people who were more likely to be religiously fundamentalists held more conspiracy theories and were less likely to follow public health guidelines about the COVID-19 epidemic (Sobol et al., 2022; Łowicki et al., 2022).
On the other hand, there are some additional socio-political and historical variables which make believers of some religions more prone to conspiracy beliefs. For example, it was suggested that in many Islamic countries, support for conspiracy beliefs is driven more by cultural and political factors related to general attitudes towards Western colonialism or Islamic anti-Semitism or anti-Zionism, and in countries where Muslims constitute minority, it results from perceived intergroup threats and shared idea that institutional authority make unfair decisions, which deprive people of their rights socioeconomic, political and social participation (Jasinskaja-Lahti et al, 2019; Bilewicz, 2022).
However, these findings are consistent with expectations, as previous research has demonstrated that individuals who identify as religious or spiritual tend to exhibit lower levels of science literacy, greater scepticism towards science, and less favourable attitudes towards science and (bio)technology (Cary et al., 2020; Evans, 2011; Johnson et al., 2015; McPhetres et al., 2020; Payir et al., 2021; Sherkat, 2011). For example, Chan (2018) showed that although the association between religiosity and various orientations towards science varies by country, on average, religiosity is negatively associated with confidence in science, trust in scientific authority under conditions of conflict with religion, faith in science, views on the moral effects of science, and interest in scientific knowledge. Religiosity was also associated with lower support for biobank donation (Broekstra et al., 2021; Sanderson et al., 2017; Sheppard et al., 2018) and higher support for conspiracies about COVID-19 (Kosarkova et al., 2022; Sobol et al., 2022).
All the above points are essential since beliefs in medical conspiracy theories significantly influence health-related behaviours, shape individuals’ reliance on conventional medicine, and affect health-seeking patterns (Lahrach & Furnham, 2017; Marques et al., 2022). For example, a study by Oliver and Wood demonstrated that while people who believe in at least three medical conspiracy theories are far more likely to take herbal supplements than people who do not believe in these theories (35% vs. 13%), they are also far less likely to be vaccinated against the flu (25% vs. 39%) (Oliver & Wood, 2014b, p. 818). Other researchers also suggest that a conspiracy belief influences people’s preferences for unconventional therapies (Bertin et al., 2020; Fournier & Varet, 2023; Ladini, 2022; Oliver & Wood, 2014a; Soveri et al., 2021) and scepticism towards screening for cancer (Sonia et al., 2022). Finally, in the context of the COVID-19 pandemic, support for medical conspiracy theories has manifested in reduced adherence to prescribed preventive measures (including personal protective equipment, social distancing, testing, isolation, quarantine, and lockdown) and vaccination reluctance among those endorsing such theories (Bierwiaczonek et al., 2022; Jones, 2022; Romer & Jamieson, 2020). These findings underscore the urgent need for tailored public health interventions that account for religious contexts and address the underlying factors contributing to medical conspiracy theory beliefs (Jabkowski et al., 2023).
Multilevel logistic regression models and a robust dataset from the Eurobarometer survey contribute to comprehensive insights into the complex relationship between religiosity and medical conspiracy theories across 37 European countries. The number of countries included in our study is undoubtedly an advantage over other research projects, as it allows us to go beyond single-country case studies (Cherniak et al., 2023), which—although necessary and valuable—do not provide an opportunity to see the relationship between religiosity and beliefs in medical conspiracy theories in a broader geographical and cultural context.
Conversely, we recommend that future research investigate the mechanisms underlying the observed associations by exploring the interplay of religious doctrines, social networks, and media influences in shaping beliefs in medical conspiracy theories. Longitudinal studies tracking changes in religiosity and medical conspiracy theory endorsements could offer insights into the evolution of these relationships over time.
Nevertheless, the critical finding of our study underscores the intricate relationship between religiosity and beliefs in medical conspiracy theories across diverse European settings, emphasising the need for tailored public health interventions that acknowledge the impact of cultural and religious contexts on health-related beliefs and behaviours. Efforts to bridge the gap between scientific evidence, public perceptions, and religious influences are crucial in promoting evidence-based healthcare practices and mitigating the adverse effects of medical conspiracy beliefs on public health. The COVID-19 pandemic has shown explicitly what the consequences of the spread of post-truth can be for the public health of entire populations.
Limitations
Our study is not without limitations. Firstly, the reliance on self-reported data introduces potential biases, such as social desirability bias or response inaccuracies, impacting the validity of the reported religiosity levels and medical conspiracy theory beliefs. Secondly, the Eurobarometer survey did not ask specific questions regarding respondents’ religious beliefs and attendance and only declared religiousness was measured. Moreover, while beliefs in the conspiracy have been associated with religious fundamentalism, the Eurobarometer survey did not use any religious fundamentalism scale. Thirdly, although the Eurobarometer survey combined “religiosity” and “spirituality” into a single construct, these categories should be distinguished. In fact, while religiosity entails holding to doctrines and customs unique to organised religion, i.e. Roman Catholic Church, and typically emphasises the value of community, belonging to shared identity and beliefs, and group worship, spirituality is more complex and flexible concept and refers to personal and subjective journey which involves a personal quest for discovering one’s inner self, meaning in life, and developing a close and intimate relationship with the sacred or transcendent, whether that be God, a supreme being, a higher power, or the spiritual realm. Thus, a personal journey for meaning does not require a community of followers or following set rules (Hill & Pargament, 2003). The identification of both categories risks obscuring important distinctions. Fourthly, while medical beliefs in conspiracy address a variety of subjects, including Big Pharma, vaccines, water fluoridation, genetically modified foods, alternative medicine, and disease denial, the Eurobarometer survey refers only to two general questions with true/false response options, which limits the generalisability of the findings and conclusions. Fifthly, operationalising medical conspiracy theories using specific survey statements might not encapsulate the entire spectrum of medical conspiracy narratives, possibly missing nuanced beliefs. While the study considers country-level contextual variables, other influential factors, such as cultural nuances, political climates, and historical contexts, are not extensively explored but might impact belief systems and medical conspiracy theory prevalence (Douglas et al., 2015; Lazić & Žeželj, 2021). Finally, the study focused on European contexts, and cultural variations beyond this continent could provide further depth to understanding these dynamics. Moreover, the multilevel regression models, while robust, involve intricate statistical analyses and only allow for descriptions of relationships, not causal explanations. Thus, the interpretation of results might be challenging for non-specialists (particularly in terms of the practical implications for public health policies), and the selection of specific variables or model specifications could affect the outcomes, warranting cautious interpretation of the findings (Jolley & Douglas, 2014).
However, despite the limitations highlighted here, this study, covering as many as 37 European countries, fills a gap in the literature on religiosity and medical conspiracy theories, thus opening new research opportunities in exploring this socially relevant issue.
Conclusions
As beliefs in conspiracy theories, including those related to medicine, are proliferating in Europe, they impact individual health-related behaviours and societies’ responses during the present pandemic caused by the novel coronavirus. By analysing data from 37 countries, both at the individual and country levels, this study adds to the growing body of evidence that religion, among other well-known factors, is a significant predictor of support for medical conspiracy theories.
While at the country level, we found significant cross-country differences in the spread of belief in conspiracy theories, this being more prevalent in the Baltic, Balkan, Southern, Central and Eastern European countries, at the individual level, we found that both confession and declared religiosity significantly influenced people’s beliefs in medical conspiracy theories. In fact, people who declared themselves to be religious—Muslims, Orthodox Christians, and Catholics, in particular—were more prone to support medical conspiracy theories. This finding is of particular importance, as many previous studies have stressed that factors such as age, gender, educational status, political orientation, and trust in science predict support for conspiracy theories. Still, the association with personal religiosity has been somewhat neglected. Thus, by identifying religion as yet another factor strongly associated with a conspiracy belief, this research suggests that future studies should focus on exploring how religion affects support for beliefs in medical conspiracy theories.
Thus, while future systematic studies on the association between religiosity and beliefs in medical conspiracy theories are needed, conducting more methodologically rigorous studies is desirable. Additionally, future studies should further investigate the link between religious fundamentalism and a broader spectrum of (medical) conspiracy theories. Finally, it is recommended to further research on inter-religious differences and precise socio-political and historical variables that make some religions more prone to support conspiracy theories.
Data availability
All data are publicly available via the GESIS Leibnitz Institute for the Social Sciences website https://doi.org/10.4232/1.13884. The data availability statement is in the main body of the manuscript.
References
-
Andrade G (2020) Medical conspiracy theories: cognitive science and implications for ethics. Med Health Care Philos 23(3):505–518. https://doi.org/10.1007/s11019-020-09951-6
-
Armfield JM (2007) When public action undermines public health: a critical examination of antifluoridationist literature. Aust N Z Health Policy 4(1):25. https://doi.org/10.1186/1743-8462-4-25
-
Bauman Z (2000) Liquid modernity. Polity Press, Cambridge
-
Beller J (2017) Religion and militarism: The effects of religiosity, religious fundamentalism, religious conspiracy belief, and demographics on support for military action. Peace Confl: J Peace Psychol 23(2):179–182. https://doi.org/10.1037/pac0000250
-
Bertin P, Nera K, Delouvée S (2020) Conspiracy beliefs, rejection of vaccination, and support for hydroxychloroquine: a conceptual replication-extension in the COVID-19 pandemic context. Front Psychol 11. https://doi.org/10.3389/fpsyg.2020.565128
-
Beyer H, Herrberg N (2023) The revelations of Q. Dissemination and resonance of the QAnon conspiracy theory among US Evangelical Christians and the role of the Covid-19 crisis. Z f ür Relig, Ges Polit 7:669–687. https://doi.org/10.1007/s41682-023-00147-2
-
Bierwiaczonek K, Gundersen AB, Kunst JR (2022) The role of conspiracy beliefs for COVID-19 health responses: a meta-analysis. Curr Opin Psychol 46:101346. https://doi.org/10.1016/j.copsyc.2022.101346
-
Bilewicz M (2022) Conspiracy beliefs as an adaptation to historical trauma. Curr Opin Psychol 47:101359. https://doi.org/10.1016/j.copsyc.2022.101359
-
Blaskiewicz R (2013) The Big Pharma conspiracy theory. Med Writ 22(4):259–261. https://doi.org/10.1179/2047480613Z.000000000142
-
Broekstra R, Aris-Meijer J, Maeckelberghe E et al. (2021) Demographic and prosocial intrapersonal characteristics of biobank participants and refusers: the findings of a survey in the Netherlands. Eur J Hum Genet 29(1):11–19. https://doi.org/10.1038/s41431-020-0701-1
-
Carstairs C (2015) Debating water fluoridation before Dr. Strangelove. Am J Public Health 105(8):1559–1569. https://doi.org/10.2105/AJPH.2015.302660
-
Cary F, Alec T, Brian K, Courtney J (2020) Biotechnology research viewed with caution globally, but most support gene editing for babies to treat disease. https://policycommons.net/artifacts/1426276/biotechnology-research-viewed-with-caution-globally-but-most-support-gene-editing-for-babies-to-treat-disease. Accessed 22 Dec 2023
-
Chan E (2018) Are the religious suspicious of science? Investigating religiosity, religious context, and orientations towards science. Public Underst Sci 27(8):967–984. https://doi.org/10.1177/0963662518781231
-
Cherniak AD, Pirutinsky S, Rosmarin DH (2023) Religious beliefs, trust in public figures, and adherence to COVID-19 health guidelines among American orthodox and non-orthodox Jews. J Relig Health 62(1):355–372. https://doi.org/10.1007/s10943-022-01718-y
-
Compton J, van der Linden S, Cook J, Basol M (2021) Inoculation theory in the post-truth era: Extant findings and new frontiers for contested science, misinformation, and conspiracy theories. Soc Personal Psychol Compass 15(6):e12602. https://doi.org/10.1111/spc3.12602
-
Davidson M (2017) Vaccination as a cause of autism—myths and controversies. Dialogue Clin Neurosci 19(4):403–407. https://doi.org/10.31887/DCNS.2017.19.4/mdavidson
-
Douglas KM, Sutton RM, Callan MJ et al. (2016) Someone is pulling the strings: Hypersensitive agency detection and belief in conspiracy theories. Think Reason 22(1):57–77. https://doi.org/10.1080/13546783.2015.1051586
-
Douglas KM, Sutton RM, Jolley D, Wood MJ (2015) The social, political, environmental, and health-related consequences of conspiracy theories: Problems and potential solutions. In: Bilewicz M, Cichocka A, Soral W (eds) The psychology of conspiracy, Routledge, London, pp. 183–200
-
Douglas KM, Uscinski JE, Sutton RM et al. (2019) Understanding conspiracy theories. Political Psychol 40(S1):3–35. https://doi.org/10.1111/pops.12568
-
Drochon H (2018) Who believes in conspiracy theories in Great Britain and Europe? In: Uschinski JE (ed) Conspiracy theories and the people who believe them. Oxford University Press, Oxford, pp. 337–346
-
Duesberg P (1992) AIDS: The alternative view. Lancet 339(8808):1547
-
European Commission (2022) Eurobarometer 95.2 GESIS, Köln. ZA7782 Datenfile Version 1.0.0. https://doi.org/10.4232/1.13884. Accessed 20 Dec 2023
-
Eurobarometer (2010) Europeans and biotechnology in 2010: Winds of change? https://europa.eu/eurobarometer/surveys/detail/755. Accessed 20 Dec 2023
-
Evans JH (2011) Epistemological and moral conflict between religion and science. J Sci Study Relig 50(4):707–727. https://doi.org/10.1111/j.1468-5906.2011.01603.x
-
Finke R, Adamczyk A (2008) Cross-national moral beliefs: The influence of national religious context. Sociol Q 49(4):617–652. https://doi.org/10.1111/j.1533-8525.2008.00130.x
-
Fournier V, Varet F (2023) Conspiracy beliefs and intention to use conventional, complementary and alternative medicines: Two vignette studies. Br J Health Psychol. https://doi.org/10.1111/bjhp.12702
-
Frenken M, Bilewicz M, Imhoff R (2023) On the relation between religiosity and the endorsement of conspiracy theories: The role of political orientation. Political Psychol 44(1):139–156. https://doi.org/10.1111/pops.12822
-
Geissler E, Sprinkle RH (2013) Disinformation squared: Was the HIV-from-Fort-Detrick myth a Stasi success? Polit Life Sci 32(2):2–99. https://doi.org/10.2990/32_2_2
-
Harambam J, Grusauskaite K, de Wildt L (2022) Poly-truth, or the limits of pluralism: Popular debates on conspiracy theories in a post-truth era. Public Underst Sci 31(6):784–798. https://doi.org/10.1177/09636625221092145
-
Heck RH, Thomas SL, Tabata LN (2013) Multilevel and Longitudinal Modeling with IBM SPSS (2nd edn.). Routledge, London
-
Heidi Oi-Yee L, Adrian B, David H, James C (2020) YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Glob Health 5(5):e002604. https://doi.org/10.1136/bmjgh-2020-002604
-
Hill PC, Pargament KI (2003) Advances in the conceptualization and measurement of religion and spirituality. Implications for physical and mental health research. Am Psychol 58(1):64–74. https://doi.org/10.1037/0003-066x.58.1.64
-
Imhoff R, Lamberty P (2020) A bioweapon or a hoax? The link between distinct conspiracy beliefs about the coronavirus disease (COVID-19) outbreak and pandemic behavior. Soc Psychol Personal Sci 11(8):1110–1118. https://doi.org/10.1177/1948550620934692
-
Imhoff R, Zimmer F, Klein O et al. (2022) Conspiracy mentality and political orientation across 26 countries. Nat Hum Behav 6(3):392–403. https://doi.org/10.1038/s41562-021-01258-7
-
Jabkowski P, Domaradzki J, Baranowski M (2023) Exploring COVID-19 conspiracy theories: education, religiosity, trust in scientists, and political orientation in 26 European countries. Sci Rep. 13(1):18116. https://doi.org/10.1038/s41598-023-44752-w
-
Jasinskaja-Lahti I, Jetten J (2019) Unpacking the relationship between religiosity and conspiracy beliefs in Australia. Br J Soc Psychol 58:938–954. https://doi.org/10.1111/bjso.12314
-
Johnson DR, Scheitle CP, Ecklund EH (2015) Individual religiosity and orientation towards science: Reformulating relationships. Sociol Sci 7(7):106–124. https://doi.org/10.15195/v2.a7
-
Jolley D, Douglas KM (2014) The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 9(2):e89177. https://doi.org/10.1371/journal.pone.0089177
-
Jones DG (2022) Religious concerns about COVID-19 vaccines: from abortion to religious freedom. J Relig Health 61(3):2233–2252. https://doi.org/10.1007/s10943-022-01557-x
-
Kalichman SC, Eaton L, Cherry C (2010) There is no proof that HIV causes AIDS”: AIDS denialism beliefs among people living with HIV/AIDS. J Behav Med 33(6):432–440. https://doi.org/10.1007/s10865-010-9275-7
-
Kosarkova A, Malinakova K, Novak L et al (2022) Religious conspiracy theories about the COVID-19 pandemic are associated with negative mental health. Int J Public Health 67. https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604324
-
Kosarkova A, Malinakova K, van Dijk JP, Tavel P (2021) Vaccine refusal in the Czech Republic is associated with being spiritual but not religiously affiliated. Vaccines 9(10):1157, https://www.mdpi.com/2076-393X/9/10/1157
-
Kwok H, Singh P, Heimans S (2023) The regime of ‘post-truth’: COVID-19 and the politics of knowledge. Discourse Stud Cult Polit Educ 44(1):106–120. https://doi.org/10.1080/01596306.2021.1965544
-
Ladini R (2022) Religious and conspiracist? An analysis of the relationship between the dimensions of individual religiosity and belief in a big pharma conspiracy theory. Ital Polit Sci Rev/Riv Ital di Sci Polit 52(1):33–50. https://doi.org/10.1017/ipo.2021.15
-
Lahrach Y, Furnham A (2017) Are modern health worries associated with medical conspiracy theories? J Psychosom Res 99:89–94. https://doi.org/10.1016/j.jpsychores.2017.06.004
-
Lazić A, Žeželj I (2021) A systematic review of narrative interventions: Lessons for countering anti-vaccination conspiracy theories and misinformation. Public Underst Sci 30(6):644–670. https://doi.org/10.1177/09636625211011881
-
Lewandowsky S, Ecker UKH, Cook J (2017) Beyond misinformation: Understanding and coping with the “post-truth” era. J Appl Res Mem Cogn 6(4):353–369. https://doi.org/10.1016/j.jarmac.2017.07.008
-
Lockie S (2017) Post-truth politics and the social sciences. Environ Sociol 3(1):1–5. https://doi.org/10.1080/23251042.2016.1273444
-
Łowicki P, Marchlewska M, Molenda Z et al. (2022) Does religion predict coronavirus conspiracy beliefs? Centrality of religiosity, religious fundamentalism, and COVID-19 conspiracy beliefs. Personal Individ Differ 187:111413. https://doi.org/10.1016/j.paid.2021.111413
-
Malcolm D (2021) Post-truth society? An Eliasian sociological analysis of knowledge in the 21st century. Sociology 55(6):1063–1079. https://doi.org/10.1177/0038038521994039
-
Marques MD, Douglas KM, Jolley D (2022) Practical recommendations to communicate with patients about health-related conspiracy theories. Med J Aust 216(8):381–384. https://doi.org/10.5694/mja2.51475
-
Mashuri A, Osteen C (2023) Threat by association, Islamic puritanism and conspiracy beliefs explain a religious majority group’s collective protest against religious minority groups. Psychol Dev Soc 35(1):169–196. https://doi.org/10.1177/09713336231152312
-
McCarthy M (2014) Nearly half of Americans believe in at least one medical conspiracy theory, survey finds. Br Med J 348:g2277. https://doi.org/10.1136/bmj.g2277
-
McPhetres J, Jong J, Zuckerman M (2020) Religious Americans have less positive attitudes toward science, but this does not extend to other cultures. Soc Psychol Personal Sci 12(4):528–536. https://doi.org/10.1177/1948550620923239
-
McPhetres J, Zuckerman M (2018) Religiosity predicts negative attitudes towards science and lower levels of science literacy. PLoS ONE 13(11):e0207125. https://doi.org/10.1371/journal.pone.0207125
-
Müller TS, De Graaf ND, Schmidt P (2014) Which societies provide a strong religious socialization context? Explanations beyond the effects of national religiosity. J Sci Study Relig 53(4):739–759. https://doi.org/10.1111/jssr.12147
-
Nally D (2022) Theorising post-truth in the COVID era. J Educ Change 23(2):277–289. https://doi.org/10.1007/s10833-022-09457-3
-
Nattrass N (2023) Promoting conspiracy theory: from AIDS to COVID-19. Glob Public Health 18(1):2172199. https://doi.org/10.1080/17441692.2023.2172199
-
Nefes TS, Aksoy O (2024) The impact of partisanship and religiosity on conspiracy-theory beliefs in Turkey. Sociol Compass 18(1):e13152. https://doi.org/10.1111/soc4.13152
-
Oliver JE, Wood T (2014a) Conspiracy theories and the paranoid style(s) of mass opinion. Am J Political Sci 58(4):952–966. https://doi.org/10.1111/ajps.12084
-
Oliver JE, Wood T (2014b) Medical conspiracy theories and health behaviors in the United States. JAMA Intern Med 174(5):817–818. https://doi.org/10.1001/jamainternmed.2014.190
-
Parmet WE, Paul J (2020) COVID-19: The first posttruth pandemic. Am J Public Health 110(7):945–946. https://doi.org/10.2105/AJPH.2020.305721
-
Pavić Ž, Šuljok A (2022) Vaccination conspiracy beliefs among social science & humanities and STEM educated people—an analysis of the mediation paths. PLOS ONE 17(3):e0264722. https://doi.org/10.1371/journal.pone.0264722
-
Payir A, Davoodi T, Cui KY et al. (2021) Are high levels of religiosity inconsistent with a high valuation of science? Evidence from the United States, China and Iran. Int J Psychol 56(2):216–227. https://doi.org/10.1002/ijop.12701
-
Pertwee E, Simas C, Larson HJ (2022) An epidemic of uncertainty: rumors, conspiracy theories and vaccine hesitancy. Nat Med 28(3):456–459. https://doi.org/10.1038/s41591-022-01728-z
-
R Core Team (2023) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
-
Robertson D, Dyrendal A (2018) Conspiracy theories and religion: superstition, seekership, and salvation. In: Uscinski JE (ed) Conspiracy theories and the people who believe them. Oxford Academic Press, Oxford, pp. 411–421
-
Romer D, Jamieson KH (2020) Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc Sci Med 263:113356. https://doi.org/10.1016/j.socscimed.2020.113356
-
Roozenbeek J, Schneider CR, Dryhurst S et al. (2020) Susceptibility to misinformation about COVID-19 around the world. R Soc Open Sci 7(10):201199. https://doi.org/10.1098/rsos.201199
-
Ruiter S, De Graaf ND (2006) National context, religiosity, and volunteering: results from 53 countries. Am Sociol Rev 71(2):191–210. https://doi.org/10.1177/000312240607100202
-
Ruiter S, Van Tubergen F (2009) Religious attendance in cross-national perspective: a multilevel analysis of 60 countries. Am J Sociol 115(3):863–895. https://doi.org/10.1086/603536
-
Sanderson SC, Brothers KB, Mercaldo ND et al. (2017) Public attitudes toward consent and data sharing in biobank research: A large multi-site experimental survey in the US. Am J Hum Genet 100(3):414–427. https://doi.org/10.1016/j.ajhg.2017.01.021
-
Shahsavari S, Holur P, Wang T et al. (2020) Conspiracy in the time of corona: Automatic detection of emerging COVID-19 conspiracy theories in social media and the news. J Comput Soc Sci 3(2):279–317. https://doi.org/10.1007/s42001-020-00086-5
-
Sheppard VB, Hurtado-de-Mendoza A, Zheng Y-L et al. (2018) Biospecimen donation among black and white breast cancer survivors: opportunities to promote precision medicine. J Cancer Survivorship 12(1):74–81. https://doi.org/10.1007/s11764-017-0646-8
-
Sherkat DE (2011) Religion and scientific literacy in the United States. Soc Sci Q 92(5):1134–1150. https://doi.org/10.1111/j.1540-6237.2011.00811.x
-
Sobol M, Zajenkowski M, Jankowski KS (2022) Religious fundamentalism, delusions, and conspiracy beliefs related to the COVID-19 pandemic. Int J Environ Res Public Health 19(15):9597. https://doi.org/10.3390/ijerph19159597
-
Sonia P, Yolanda B, Alexandra M et al. (2022) Everything causes cancer? Beliefs and attitudes towards cancer prevention among anti-vaxxers, flat earthers, and reptilian conspiracists: online cross sectional survey. BMJ 379:e072561. https://doi.org/10.1136/bmj-2022-072561
-
Soveri A, Karlsson LC, Antfolk J et al. (2021) Unwillingness to engage in behaviors that protect against COVID-19: the role of conspiracy beliefs, trust, and endorsement of complementary and alternative medicine. BMC Public Health 21(1):684. https://doi.org/10.1186/s12889-021-10643-w
-
Speed E, Mannion R (2017) The rise of post-truth populism in pluralist liberal democracies: Challenges for health policy. Int J Health Policy Manag 6(5):249–251. https://doi.org/10.15171/ijhpm.2017.19
-
Tonković M, Dumančić F, Jelić M, Čorkalo Biruški D (2021) Who believes in COVID-19 conspiracy theories in Croatia? Prevalence and predictors of conspiracy beliefs. Front Psychol 12. https://doi.org/10.3389/fpsyg.2021.643568
-
Uscinski JE, Enders AM, Diekman A et al. (2022) The psychological and political correlates of conspiracy theory beliefs. Sci Rep. 12(1):21672. https://doi.org/10.1038/s41598-022-25617-0
-
Uscinski JE, Enders AM, Klofstad C et al. (2022) Have beliefs in conspiracy theories increased over time? PLoS ONE 17(7):e0270429. https://doi.org/10.1371/journal.pone.0270429
-
Uscinski JE (2018) Conspiracy theories and the people who believe them. Oxford University Press
-
Uscinski JE Enders AM (2023) Conspiracy theories: a primer. Rowman & Littlefield, Lanham
-
van Prooijen J-W (2018) The psychology of conspiracy theories. Routledge, London
-
van Prooijen J-W, Douglas KM (2017) Conspiracy theories as part of history: the role of societal crisis situations. Mem Stud 10(3):323–333. https://doi.org/10.1177/1750698017701615
-
Wakefield AJ, Murch SH, Anthony A et al. (1998) RETRACTED: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Lancet 351(9103):637–641. https://doi.org/10.1016/S0140-6736(97)11096-0
-
Walkowiak MP, Domaradzki J, Walkowiak D (2022) Better late than never: predictors of delayed COVID-19 vaccine uptake in Poland. Vaccines 10(4):528, https://www.mdpi.com/2076-393X/10/4/528
-
Wolfe RM, Sharp LK (2002) Anti-vaccinationists past and present. Br Med J 325(7361):430. https://doi.org/10.1136/bmj.325.7361.430
-
Yendell A, Herbert D (2022) Religion, conspiracy thinking, and the rejection of democracy: evidence from the UK. Polit Gov 10(4):229–242. https://doi.org/10.17645/pag.v10i4.5904
Author information
Authors and Affiliations
Contributions
All authors equally contributed to the study’s conception, design, analysis, and writing. All authors approved the submitted version. PJ conducted statistical analysis, prepared Tables 1 and 2, Figures 1, 2, and 3, and wrote the main manuscript text. JD and MB wrote the main manuscript text and worked on the discussion and conclusions. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study exclusively used publicly available aggregate data sets and published research; hence, no ethics approval was required.
Informed consent
As this study utilised publicly accessible, anonymised data and did not involve the participation of human subjects, the acquisition of informed consent was not a requisite component.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article
Cite this article
Jabkowski, P., Domaradzki, J. & Baranowski, M. Religiosity and beliefs in medical conspiracy theories in 37 European countries during the COVID-19 pandemic.
Humanit Soc Sci Commun 12, 434 (2025). https://doi.org/10.1057/s41599-025-04781-4
-
Received: 20 October 2024
-
Accepted: 18 March 2025
-
Published: 26 March 2025
-
DOI: https://doi.org/10.1057/s41599-025-04781-4


