Not-so-straightforward links between believing in COVID-19-related conspiracy theories and engaging in disease-preventive behaviours | Humanities and Social Sciences Communications
Procedures
To test our predictions, we conducted a repeated cross-sectional survey across six-time-points in the United States, covering the period from early February (mild stage of the outbreak: 11 confirmed cases in the U.S.) to late March (severe stage of the outbreak: 68,440 in the U.S.) with a survey conducted every ten days. This time frame was decided a priori to capture variations in the severity of the COVID-19 outbreak in the U.S. as much as possible given our limited funding and resources. We will provide validation of this time frame in the Results section.
Participants
We targeted 250 adult U.S. participants at each time-point. This sample size has 80% statistical power to detect a weak-to-moderate correlational strength with alpha at 0.05 level at each time-point. To ensure that the sample at each time-point was comparable to those at other time-points, we recruited participants from the same participant pool. In total, we recruited 1515 participants for all six time-points via Cloudresearch (Litman et al., 2017), a research-tool platform that recruits participants from Amazon Mechanical Turk. The data collection procedures and research materials were reviewed and approved by the Committee on Research Practices of the university affiliated with the corresponding authors (Reference number: SBRE-19-294). All participants gave their consent first and then completed the online survey, only once each (see also Supplementary Information for the details of the consent form and debriefing note). We included three attention-check items following the recommendation of past studies (e.g., Curran, 2016). Specifically, participants were required to provide exactly the same answer as instructed (e.g., “This is an attention-check item; please click “strongly agree” to pass this attention check.”). Seven participants failed all three attention-check items and were removed from the subsequent analyses. Supplementary Table 1 shows the sample characteristics of the participants at each time-point. Results showed high similarities in the demographic characteristics of the samples across the six time-points, suggesting that it is possible to compare findings across these samples.
Measures
Belief in COVID-19 Conspiracy Theories
To create the risk-acceptance and risk-rejection types of conspiracy-theory items, we collected frequently mentioned conspiracy theory narratives from news reports (e.g., BBC News), social media (e.g., Facebook, Twitter), and fact-checking sites (e.g., Snopes.com, Fackcheck.org) in January 2020. Based on the narratives collected, we generated five items to capture risk-acceptance conspiracy theories: “The outbreak of the novel coronavirus is caused by some organisations and countries on purpose in order to fulfil their secret plans;” “The spread of the novel coronavirus is caused by some people intentionally;” “The novel coronavirus is a bioweapon created by the Chinese government;” “The novel coronavirus was stolen by Chinese spies from a laboratory in Canada;” and “The Chinese government has covered up the true number of people infected by the novel coronavirus.” We generated two items to capture risk-rejection conspiracy theories: “In reality, the novel coronavirus is similar to influenza. It is just that some organisations and people purposefully exaggerate its severity;” and “The novel coronavirus actually does not spread easily among humans; it is being used as an excuse to control the influx of Chinese people by foreign countries.” Participants reported on an 11-point scale (0 = not true at all to 10 = completely true) to indicate the extent to which they believed each statement to be true. These two types of items resemble the COVID-human-made and COVID-hoax items used in Imhoff and Limberty (2020) and Sternisko et al. (2020). To validate these conspiracy-theory items, we conducted a social media-engagement search in a retrospective manner (for details, see Supplementary Information; see also Supplementary Tables 7 and 8), and found that these items have sufficient coverage of popular real-life conspiracy theories that were circulating on social media from January to March 2020. Footnote 1 We computed a mean score for each type of conspiracy theory.Footnote 2 Supplementary Table 2 shows the mean, standard deviation, and reliability of the measures. Footnote 3
Our generation of the items was limited by two major constraints. First, the social discourse regarding the novel coronavirus and its spread was still evolving in January 2020 when we created the items. Some of the conspiracy theories, such as the 5G- and Bill Gates-related conspiracy theories, were not yet widely circulated at that stage, and thus we have not included them in our measure. Second, incidentally, there were many more conspiracy theories portraying COVID-19 as a human-caused crisis than as a hoax during that period. Accordingly, we included more risk-acceptance than risk-rejection items in our measure.
Risk perception
We identified three items to capture individuals’ perceived risk of getting infected with COVID-19 from past studies on the perceived risk of infectious disease (e.g., Piltch‐Loeb et al., 2019). Participants indicated the likelihood with which they believed someone in their local community, their family, or themselves to be to contract COVID-19 on a 7-point scale (1 = not at all likely to 7 = extremely likely). We computed a mean score based on the three items. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Negative emotions toward COVID-19
We identified eight emotional-state items to capture people’s feelings toward COVID-19. Five of the items were negative emotions: afraid, threatened, anxious, tense, and disgusted. Three of the items were positive emotions: optimistic, calm, and hopeful. Participants reported on a 7-point scale (1 = not at all to 7 = extremely) to indicate their feelings toward the COVID-19 outbreak. Confirmatory factor analysis showed a good fit for a two-factor solution (CFI = 0.990, TLI = 0.983, RMSEA = 0.060). We computed a mean score for negative emotions and positive emotions, respectively. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measures.
We did not include positive emotions toward COVID-19 in our main analysis because we did not theorise a causal impact of such positive emotions on disease-preventive behaviours. On the one hand, it is plausible that positive emotions empower people to engage more in disease-preventive behaviours. On the other hand, positive emotions may reassure people that COVID-19 does not represent a real threat. Consequently, positive emotions could possibly impede people from engaging in disease-preventive behaviours. We explored this issue empirically and found that positive emotions toward COVID-19 had a slight negative correlation with disease-preventive behaviours (r = −0.05, N = 1508). We also performed a supplementary analysis to probe the relationship between belief in COVID-19 conspiracy theories and positive emotions toward COVID-19 (see Supplementary Table 6). Belief in the risk-acceptance type of COVID-19 conspiracy theory was unrelated to positive emotions toward COVID-19, whereas belief in the risk-rejection type of COVID-19 conspiracy theory was positively related to positive emotions toward COVID-19. Furthermore, our results remained consistent when we included positive emotions toward COVID-19 as a covariate in the parallel mediation analysis. Positive emotions toward COVID-19 were non-significant in predicting disease-preventive behaviours in the mediation analysis (b = 0.02, SE = 0.01, p = 0.189, 95% CI = [−0.01, 0.05]).
Disease-preventive behaviours
We identified 10 disease-preventive behaviours based on the recommendations from the U.S. Centers for Disease Control and Prevention (CDC) and those recommended in countries that had earlier outbreaks (e.g., the Chinese Center for Disease Control and Prevention). Specifically, participants reported on a five-point scale (1 = never to 5 = always) to indicate how frequently they performed the following behaviours in the past week: “Wear a mask in public places,” “Wash hands with soap and water for at least 20 s or use an alcohol-based hand sanitiser,” “Wash hands before touching eyes, nose, and mouth,” “Avoid leaving home,” “Change clothes and wash hands when coming back from outside immediately upon returning home,” “Avoid crowded areas,” “Pay close attention to household and personal hygiene,” “Avoid travelling to areas where the novel coronavirus is prevalent,” “Avoid taking public transport,” and “Keep monitoring one’s own body temperature.” We computed a mean score to indicate people’s overall engagement in disease-preventive behaviours. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Covariates
Institutional trust
Conceptually, conspiracy theories may also lead to reduced trust in scientists, governments, and medical institutions, and thus may make people less likely to adopt recommendations from these agents (Earnshaw et al., 2019; Sell et al., 2020). Therefore, we also controlled for the effect of institutional trust to rule out this alterative mechanism. To this end, we created a four-item measure of trust in U.S. institutions based on past studies (e.g., Piltch‐Loeb et al., 2019). Participants reported on a 7-point scale (1 = not at all to 7 = extremely) to indicate the extent to which they were confident in scientists’, medical experts’, the U.S. government’s, and the CDC’s ability to control the spread of COVID-19. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Political ideology
Previous research (e.g., Calvillo et al., 2020; Georgious et al., 2020; Uscinski et al., 2020) suggested that political ideology may be related to COVID-19 conspiracy beliefs, risk perception, and disease-preventive behaviours. Although it would be interesting to study the effects of political ideology systematically, it is beyond the scope of the current research. We thus controlled for the effects of political ideology. Participants were asked to report the extent to which they endorse liberal and conservative ideologies, respectively. As these two items were strongly correlated (r = −0.78, N = 1508), we computed an average score to represent political ideology, with higher scores indicating higher levels of endorsement of conservative ideology.
Demographic information
We also included demographic variables (gender, age, education level, and annual household income) as covariates; participants reported their gender (1 = male and 0 = female), age, education level (1 = some elementary school or below, 2 = elementary school, 3 = middle school, 4 = high school or equivalent, 5 = some college/associate degree, 6 = bachelor’s degree, 7 = master’s degree, and 8 = professional or Ph.D), and annual household income (1 = less than $10,000; 2 = $10,000 to $39,999; 3 = $40,000 to $69,999; 4 = $70,000 to $99,999; and 5 = $100,000 or more). Participants also indicated their subjective socio-economic-status on a ladder of social-economic status (1 = lowest status to 10 = highest status), ethnicity and political party affiliation; these variables were used to gauge the background characteristics of the six samples.
Supplementary Table 1 shows the sampling characteristics. As shown, the sample characteristics of the participants at each time-point were highly similar, suggesting that it is possible to compare findings across the six samples.
Statistical analysis
To test our hypotheses, we conducted three sets of analysis with SPSS 25.0. First, we conducted a zero-order correlation analysis to test the bivariate relationships among the key variables in the pooled sample (all six time-points) and for each time-point separately. We used the “ggplot” package of R to visualise these bivariate associations for each time-point (see Figs. 1 and 2).
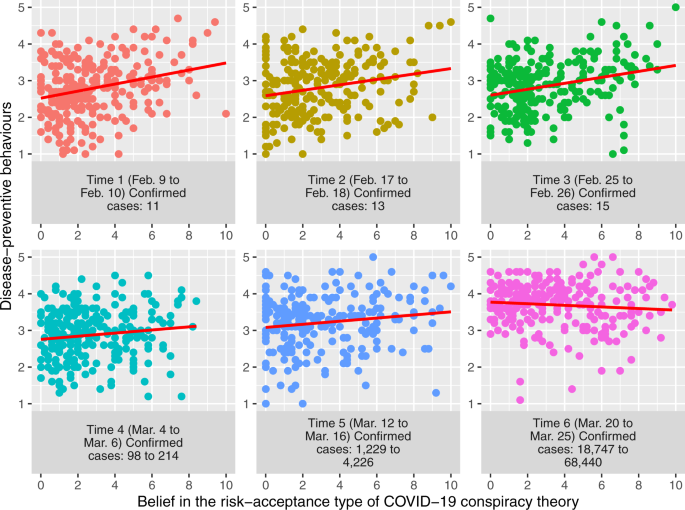
Note. The scatterplot illustrates the bivariate relationship between belief in the risk-acceptance type of COVID-19 conspiracy theories (x-axis; ranged from 0 to 10) and disease-preventive behaviours (y-axis; ranged from 1 to 5) across the six-time points of data collection. The red line illustrates the linear trend of the bivariate relationship.
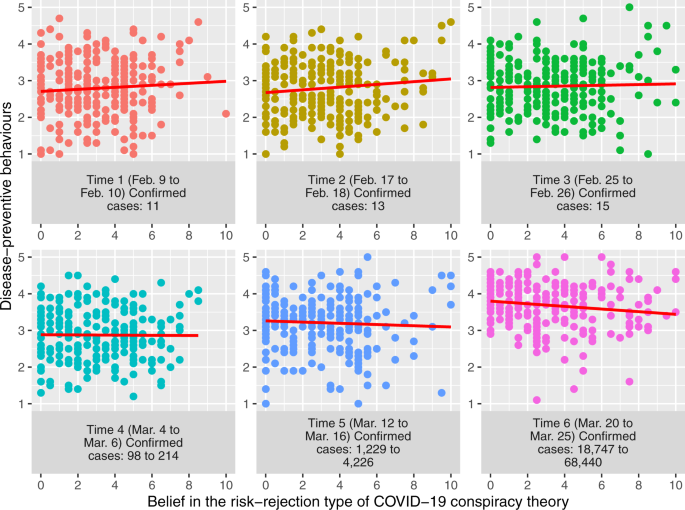
Note. The scatterplot illustrates the bivariate relationship between belief in the risk-rejection type of COVID-19 conspiracy theories (x-axis; ranged from 0 to 10) and disease-preventive behaviours (y-axis; ranged from 1 to 5) across the six-time points of data collection. The red line illustrates the linear trend of the bivariate relationship.
Next, we conducted a parallel mediation analysis using the SPSS Macro application PROCESS (Hayes, 2013), since we hypothesised both risk perception and negative emotions to be simultaneously mediating the relationship between conspiracy-theory beliefs and disease-preventive behaviour. The PROCESS application enabled researchers to estimate the indirect effects of independent variables via multiple mediator variables simultaneously and generated bootstrap estimates for these indirect effects (Hayes, 2013). In this analysis, we included the extent of believing in the two types of conspiracy beliefs (risk acceptance and risk rejection) as the independent variables, risk perception and negative emotions toward COVID-19 as the mediator variables, and disease-preventive behaviours as the outcome variable. This proposed mediation chain rests on the theoretical assumptions that (1) conspiracy theories have an implication for people’s evaluation of risk associated with an entity (in this case, COVID-19/SARS-CoV-2), and (2) such evaluation influences people’s engagement in health-related behaviour. Past studies have offered initial support to these assumptions with experimental design (e.g., Jolley and Douglas, 2014; Sheeran et al., 2014). Additionally, it would be crucial to rule out alternative mechanisms and to control for potential confounding variables in the proposed mediation analysis. Therefore, we controlled for the covariates noted above, including institutional trust, political orientation, and demographic variables.
Last, we explored how the hypothesised relationship may vary across different stages of the COVID-19 outbreak. We compared the strength of the relationship by treating the stage of the outbreak as the moderator variable and testing its effect using multiple regression analysis. We coded the stage of the COVID-19 outbreak as a continuous variable (1 = Time 1 to 6 = Time 6). To facilitate the interpretation of the moderation effect, we standardised both the independent variables (i.e., the two types of conspiracy beliefs) and the moderator variable (i.e., stage) when computing the interaction terms (i.e., conspiracy beliefs × stage). We conducted two multiple regression analyses with risk perception and negative emotions as the respective outcome variables. We used the “ggplot” package of R to illustrate the bivariate relationship between the two types of conspiracy-theory beliefs and risk perception or negative emotions (see Supplementary Figs. 1 to 4). We further explored whether or not the indirect effects of conspiracy-theory beliefs via risk perception and negative emotions on disease-preventive behaviours would vary across stages by conducting a moderated mediation analysis with PROCESS (Hayes, 2013; see also Preacher et al., 2007).


