Covid Misinformation: 20 Questions They Don’t Want to Answer

I can’t get a single one of these questions answered. I promise to stop spreading misinformation if you can just publicly answer just these questions with truthful and accurate answers.
An open letter to the White House, Surgeon General Murthy, Twitter censors, Medium censors, LinkedIn censors, YouTube censors, the medical community, the mainstream media, all members of US Congress, world leaders, all public health officials anywhere in the world, all “fact checker” organizations, and members of the California legislature especially Assemblymember Evan Low and Senator Dr. Richard Pan.
Dear folks,
I know you want to stop COVID misinformation. I agree. It’s a problem.
In my view, you are the ones spreading it, not me.
Unfortunately, not everyone sees it the same way. According to CCDH, who is arguably a world authority on misinformation spreaders (they created the original Disinformation Dozen list relied on by the White House), I’m one of the worst offenders: I’m #3 on their list.
The problem I have is simple: the data clearly shows that it is the CDC and other government agencies that are spreading misinformation, not me.
In order to resolve the conflict, I’m going to make the following offer in good faith: I will happily stop spreading “misinformation” if you all would just take a few minutes to answer a few questions for me. Fair enough? Will you do that?
If not, please tell me why not since this is your only chance of convincing people like me to get the jab.
I know this is important to you because you have a list of misinformation spreaders you want to silence. Just answer all these questions and you’ll silence us (the right way).
Here are my questions:
- Why no debates? Why won’t any mainstream doctors or scientists or public health officials (or any other health authority for that matter) debate me or any of my colleagues in a live, recorded debate? I even offer some people (members of the ACIP and VRBPAC committees) $1 million just to come to the debate table and it made no difference. We can’t even get any of them to propose any ground rules that they will accept! For example, Professor Makary proposed debate terms (which weren’t a debate) and then ignored me when I tried to accept them.
- VAERS safety signals flashing red since January 2021. How could the CDC and the FDA possibly miss all the safety signals in VAERS which have been flashing red since January 2021 for thousands of symptoms, some elevated by 1,000X or more? Why did they ignore all attempts to bring this to their attention (if it wasn’t already obvious). They clearly must have known in January that the data coming in didn’t match the claims in the clinical trials.
- Risk benefit calculation. I have more than 10 methods that show that over 150K people have been killed by the vaccine and the Pfizer trial showed we’d save 1 life from COVID for every 22,000 vaccinated. So after vaccinating 220M people, we kill 150,000 people or more and we save 10,000 lives. If this is wrong, where is the mistake and what are the correct numbers?
- Why no investigation into Maddie de Garay? Why did the FDA not investigate the Maddie de Garay case after agreeing to look into it? Why is the press silent on this as well? She was 12 years old in the Pfizer clinical trial and became paralyzed less than 24 hours after injection. Why were her symptoms reported as mild abdominal pain and not paralysis? What is causing her to now progress to being a quadriplegic? And if her symptoms weren’t caused by the vaccine (as claimed by the “fact checkers,” then why are her symptoms virtually identical to other vaccine victims and not explainable any other way?
- More people died who took the drug than those who didn’t take the drug. The Pfizer 6 month study showed that more people died who got the drug than who got the placebo (they conveniently forgot to mention this in the abstract or conclusion). Isn’t it supposed to be the other way around? Where is the RCT showing an all-cause death benefit? See this article for updated numbers in the pre-unblinding phase showing 21 dead who took the drug vs. 17 dead who took the placebo. And how was Pfizer certain that none of the people who got the drug was killed by the vaccine? What tests were done during the autopsies that exonerated the drug? These tests were never revealed and they are still being kept hidden for some odd reason. Since the vaccine wasn’t the cause, why not make the autopsy reports and tests done public that prove this?
- Elevated myocarditis rates. How is a 559-fold increase in the reporting rate of myocarditis in VAERS (see slide 19) considered to be a “slightly elevated risk” of myocarditis? Why wasn’t this noticed in January 2021? How did the CDC completely miss this signal (they admitted it was the DoD who spotted it). How do you explain 4 cases of myocarditis at the Monte Vista Christian School (with only 800 students, half of them male and perhaps half of those not vaccinated)? That’s a 1 in 50 rate. Is that just bad luck? And how is it possible that multiple military doctors I’ve asked about the rates in the military both give me numbers over 1%? Am I just unlucky?
- How do you explain Schirmacher’s study? Dr. Peter Schirmacher, one of the world’s top pathologists, reported that in 40 cases examined 2 weeks after vaccination, the vaccine killed 30% to 40% of them. Immediately after he reported this, his family was threatened if he spoke out. So Dr. Schirmacher has been silenced. See my article for details. Do you support intimidation techniques to silence legitimate scientists with dissenting views? The Federal Association of German Pathologists has called for autopsies, but the government has silenced them as well. Do you support my call for autopsies? If not, why not? Also, Schirmacher’s results have been validated by Bhakti and Burkhardt. Did all of them get it wrong? How were they fooled?
- What is causing the telltale clots? Embalmers have seen odd blood clots, never before seen before the vaccines rolled out, in up to 93% of cases. These are not normal clots and have never been seen before the vaccines rolled out. What are they caused by and why are they killing so many people?
- Excess deaths. What’s causing the excess deaths observed by insurance companies? Insurance company deaths rose in Q3 and Q4 of 2021 at the same time the boosters rolled out. The fact checkers say it is due to COVID, but the data doesn’t line up which they fail to point out. Delta started in June and was 93% by August. You’d never know that from the graph:
 10. The more you vaccinate, the worse the outcomes. Why do over 10 studies (including one covering 145 countries) all show that the more we vaccinate, the worse the infection and fatality rates? Since nobody has been able to refute any of these studies, shouldn’t we at least put the mandates temporarily on hold until the studies are refuted?
10. The more you vaccinate, the worse the outcomes. Why do over 10 studies (including one covering 145 countries) all show that the more we vaccinate, the worse the infection and fatality rates? Since nobody has been able to refute any of these studies, shouldn’t we at least put the mandates temporarily on hold until the studies are refuted?
11. Negative efficacy. The latest UK government report shows that for most age groups, you are now more than 3 times more likely to get COVID if you are triple vaccinated compared to the unvaccinated. It seems the more you vaccinate, the worse the disparity. It’s clearly tied to the number of vaccinations. How do you explain this if the vaccines are protective?
 12. CDC paper admits to negative vaccine efficacy. This is big. Finally, a paper by nine CDC authors published in JAMA in January 2022 (Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants) shows in Fig. 3 that the vaccines create negative efficacy for Omicron at month 7, just like the Denmark study showed too (in Denmark it was after 3 months). In other words, the CDC authors admit that the vaccines make you more likely to get Omicron starting in month 7. Isn’t this contrary to what the CDC has been telling us? The vaccines aren’t supposed to make things worse, right?
12. CDC paper admits to negative vaccine efficacy. This is big. Finally, a paper by nine CDC authors published in JAMA in January 2022 (Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants) shows in Fig. 3 that the vaccines create negative efficacy for Omicron at month 7, just like the Denmark study showed too (in Denmark it was after 3 months). In other words, the CDC authors admit that the vaccines make you more likely to get Omicron starting in month 7. Isn’t this contrary to what the CDC has been telling us? The vaccines aren’t supposed to make things worse, right?
13. VAERS underreporting factor. What is the URF for VAERS this year? Why didn’t anyone calculate it? Why didn’t the FDA simply admit they don’t know what it is when asked by a reporter? Why does John Su never talk about the proper URF when he talks about the VAERS data? He knows how to calculate the URF since he was one of the authors on the CDC paper for how to do this. So why is he silent?
14. How can you do risk benefit calculation without estimating the VAERS URF? This is elementary, yet none of the outside committee members of the CDC or FDA ever asks about this. Why not? I keep bringing this up in my public testimony, but they just ignore me.
15. Pfizer Phase 3 trial exclusions. How do you explain the gaming in the Pfizer trial on exclusions (311 vs. 60)? (see Slide 65). That couldn’t have happened by chance. And while you have that slide deck open, if you can answer any other questions in that deck, that would be super helpful.
16. Every randomized trial shows masks make no difference at all. If masks work, then how come the graph for purple cloth masks in the Bangladesh studyshowed absolutely no effect and why did they omit this graph from the published paper? I read through all 111 pages and couldn’t find the graph. Not only did they omit the graph, but nowhere in the paper did they point out that the purple cloth masks had no effect. Isn’t that scientific fraud? Also, if masks work, then why isn’t there any data supporting the mask policy in Israel?
17. Why don’t we have any autopsies done by a competent authority? Why don’t we just do autopsies of 100 people who died within 2 weeks of vaccination? We can have people like Peter Schirmacher, Ryan Cole, Sucharit Bhakdi, and Arne Burkhardt observe this work. That would settle the argument and end the vaccine hesitancy for sure.
18. Why is there a 5% rate of neurological damage after vaccination? If the vaccines are perfectly safe, then how do you explain how a California neurologist can have 1,000 vaccine injured in their practice of 20,000 patients. That’s a 5% neurological injury rate. This closely matches the vaccine injury rate discovered by the Israeli Ministry of Health (which was 4.5%).
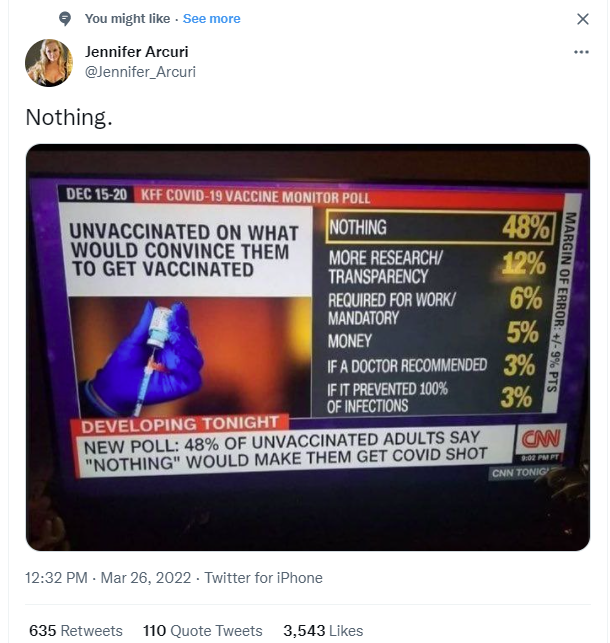
19. How do you explain this data?
20. Can you answer any of the questions on this list?
I look forward to hearing from you. I’d love to get back to technology.
Bonus questions:
- FDA’s Steven A. Anderson. He promoted himself as the top guy at the FDA on safety in his slide presentation on October 22, 2020. This was the famous presentation with Slide 17 which was a list of adverse events that was skipped over quickly. It’s remarkable how well it matched up with the safety signals that showed up in VAERS in January after the vaccines rolled out. I reached out to him multiple times by phone and email when the VAERS data showed clear safety signals. He ignored all attempts. This seems like really odd behavior for someone who is obsessed with finding a safety signal. He has never found a single safety signal himself, so when he gets a call from anyone who claims there might be a signal, how can he ignore it? He should be embracing it, right?
- Brook Jackson. Watch the video. Explain to me why there isn’t an independent investigation into the allegations in this video. And how is it possible that the day after Brook went to the FDA that she was fired from her position?
- Vaccine mandates: In Santa Clara County, they mandate vaccination for first responders. But vaccinated and unvaccinated first responders get COVID at the same rates in Santa Clara County, so why is vaccination mandated?
- Informed consent. A military doctor briefs 3,000 soldiers on the vaccine for 30 minutes and 99.8% refuse the jab. Nothing he said was false, but the doctor is relieved of duty. So if the vaccine is so safe and effective, why doesn’t anyone want to take it?
- UVGI technology. Why wasn’t UVGI technology (ultraviolet light) recommended by the CDC when the outbreak happened? Why aren’t they saying anything about it now? It’s quite effective everywhere it has been deployed as far as I’m aware. Industrial hygienists have been using this technology for their clients since early 2020. Here’s a note I received:
I know the CDC had a page early on that had controls listed in the various control categories but I haven’t seen anything this specific about prioritizing engineering controls like this, especially with the UVGI technology. We started rolling that tech option out to our clients in 2020. Nobody in government was touting UVGI tech at all. We’ve had that in our office since 2020 and have seen first hand how successful that option is. Our UVGI equipment is set to sanitize the air and surfaces every 6 minutes. Though we had infected people in our office at times, there was never an outbreak. Clients that implemented this system had similar success. This would’ve been a game changer for schools, instead of them shutting down and putting PPE on kids. It’s been difficult to watch this buffoonery from public health officials who are clearly out of their lane of expertise.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram, @globalresearch_crg and Twitter at @crglobalization. Feel free to repost and share widely Global Research articles.
Featured image is from Children’s Health Defense


