NY Times Latest to Mislead Public on New Ivermectin Study
Guest Post by
The New York Times on Wednesday sent an email to subscribers titled: “Breaking News: Ivermectin failed as a Covid treatment . . .” The Times was referring to a study in the New England Journal of Medicine, covered March 18 by The Wall Street Journal. In both cases, the newspapers failed to provide an accurate critical analysis of the study.
The New York Times on Wednesday sent an email blast to subscribers with the subject line: “Breaking News: Ivermectin failed as a Covid treatment, a large clinical trial found.”
The Times was referring to a study I wrote about, that same day, for The Defender.
My article called out the Wall Street Journal for its March 18 reporting on the same study — before the study was even published — for its failure to provide an accurate, critical assessment of the study.
The study in question — “Effect of Early Treatment with Ivermectin among Patients with Covid-19” — was officially published Wednesday in the New England Journal of Medicine (NEJM).
In it the authors concluded:
“Treatment with ivermectin did not result in a lower incidence of medical admission to a hospital due to progression of Covid-19 or of prolonged emergency department observation among outpatients with an early diagnosis of Covid-19”
The Times did not critique the study itself, but quoted the opinion of Dr. David Boulware, an infectious-disease expert at the University of Minnesota:
“There’s really no sign of any benefit. Now that people can dive into the details and the data, hopefully that will steer the majority of doctors away from ivermectin towards other therapies.”
Yes. Let us dive into the details and the data and see where it “steers” us, shall we?
A closer look at the details
The NEJM study took place in Brazil between March 23 and Aug. 6, 2021.
The study examined 1,358 people who expressed symptoms of COVID-19 at an outpatient care facility (within seven days of symptom onset), had a positive rapid test for the disease and had at least one of these risk factors for severe disease:
- Age over 50
- Hypertension requiring medical therapy
- Diabetes mellitus
- Cardiovascular disease
- Lung disease
- Smoking
- Obesity
- Organ transplantation
- Chronic kidney disease (stage IV) or receipt of dialysis
- Immunosuppressive therapy (receipt of ≥10 mg of prednisone or equivalent daily)
- Diagnosis of cancer within the previous 6 months
- Receipt of chemotherapy for cancer.
Young and healthy individuals were not part of this study.
Both vaccinated and unvaccinated individuals were included in the study. The percentage of vaccinated participants in each group was not specified. Note that by choosing not to identify vaccination status as a confounding variable the authors are implying that vaccines are playing no role in preventing hospitalization.
The 1,358 subjects were divided into two equally sized groups that were relatively well-matched and randomized to receive either a three-day dose of placebo or a three-day course of ivermectin at 400 mcg/kg.
The primary outcome was hospitalization due to COVID-19 within 28 days after randomization or an emergency department visit due to clinical worsening of COVID-19 (defined as the participant remaining under observation for >6 hours) within 28 days after randomization.
How researchers were able to conclude ‘no benefit’ despite signs to the contrary
The study’s authors wrote:
“100 patients (14.7%) in the ivermectin group had a primary-outcome event (composite of hospitalization due to the progression of COVID-19 or an emergency department visit of >6 hours that was due to clinical worsening of COVID-19), as compared with 111 (16.3%) in the placebo group (relative risk, 0.90; 95% Bayesian credible interval, 0.70 to 1.16).”
In other words, a greater percentage of placebo recipients required hospitalization or observation in an emergency department than those who received Ivermectin.
The authors of the study broke it down by subgroups here:
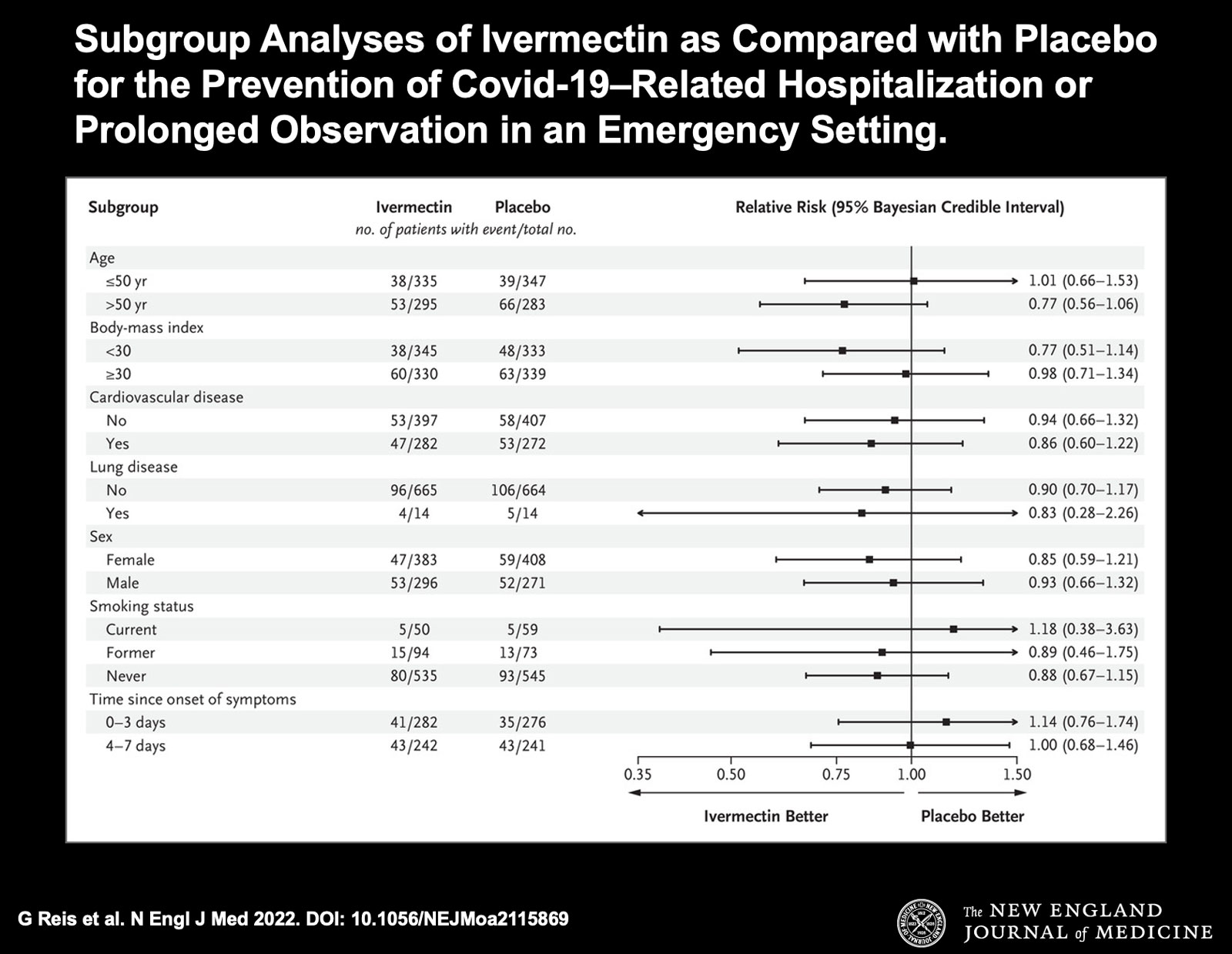
As is demonstrated in nearly every subgroup, the Ivermectin recipients fared better than those who received the placebo.
However, these data were not statistically significant given the size of the study.
This is how the authors were able to conclude there was no benefit to ivermectin use in preventing hospitalization in high-risk patients in their study.
Patients were under-dosed, some didn’t follow instructions
As it stands, the study The New York Times and The Wall Street Journal declared as proof of the uselessness of ivermectin in treating COVID-19 is actually quite promising — contrary to what their headlines told readers.
The dosing protocol advised by the Frontline COVID-19 Critical Care Alliance (FLCCC) includes a five-day course of ivermectin at 600 micrograms per kilogram of body weight for people with risk factors such as those possessed by participants in the study.
Instead, the investigators behind the NEJM study chose a much lower dose, 400mcg per day for only three days. This represents less than half of the total dose that has been shown to be effective in practice.
Furthermore, despite acknowledging that studies have shown some indication that the bioavailability of ivermectin increases when taken with food, especially a fatty meal, participants in the trial were instructed to take the medicine on an empty stomach.
In other words, the patients were significantly under-dosed — and yet a positive effect of the drug was emerging, though not statistically significant given the size of the study.
Also of note, the investigators chose to include emergency room visits with hospitalizations for COVID. Clearly, six hours of observation in an ER is a significantly different outcome than a hospitalization that may last a night or much longer.
When excluding the ER visits from the primary outcome and examining only hospitalizations, the ivermectin cohort had even less risk of an outcome, i.e. the relative risk was 0.84 vs 0.9 when ER visits and hospitalization were grouped together.
Perhaps the most glaring deficiency of the study is the low number of placebo recipients who actually followed the study’s protocol:
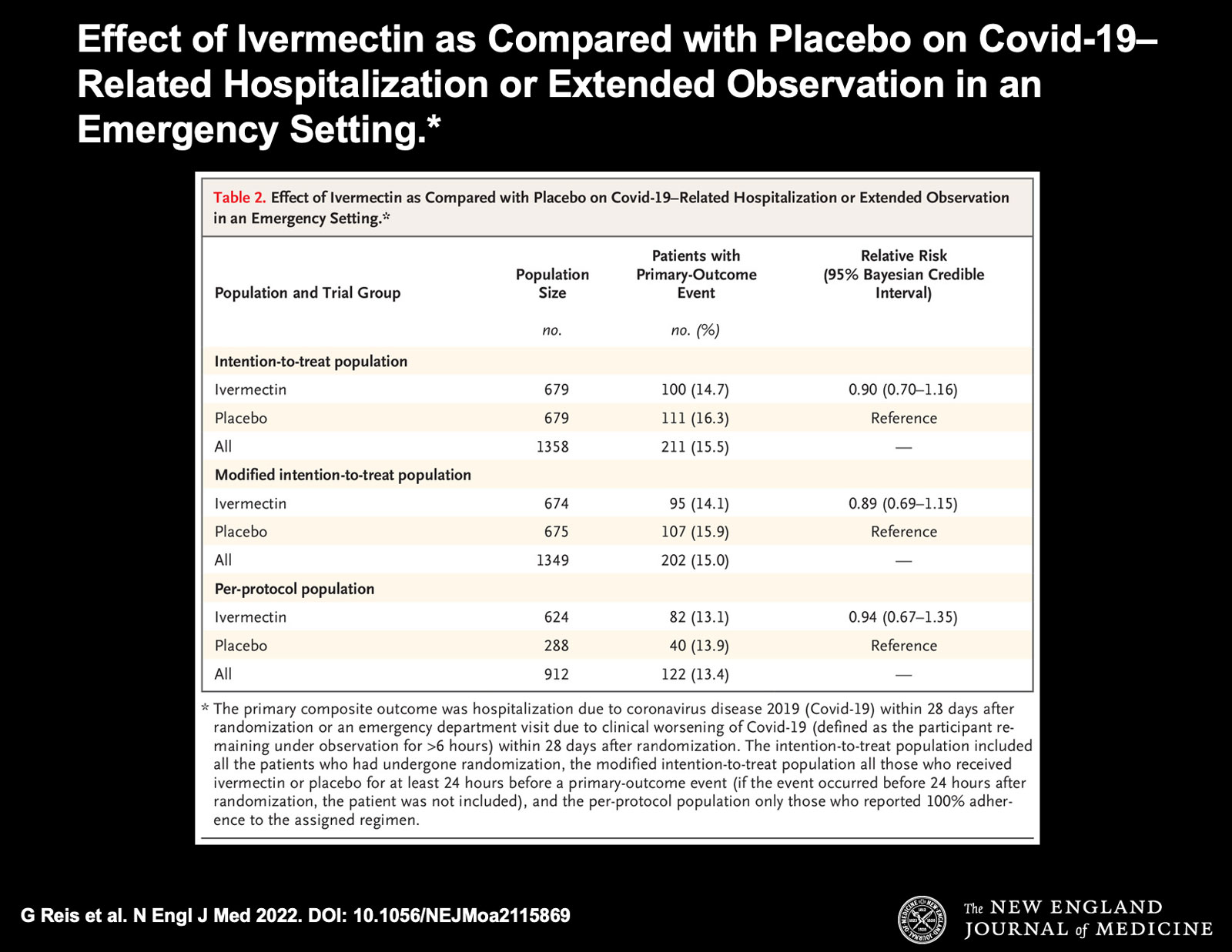
Only 288 of 679 participants randomized to receiving the placebo reported 100% adherence to the study protocol. Nearly 400 didn’t.
Why not? We asked Dr. Meryl Nass, an internist and member of the Children’s Health Defense scientific advisory committee.
Nass told The Defender:
“Presumably they knew the difference between ivermectin and placebo, and the placebo subjects went out and bought ivermectin or something else … but whatever they did, they didn’t bother with the pills they were given.
“So, it was not actually a double-blinded trial. Yet the 391 people who didn’t take the placebo but did something else were included in two of the three calculations of ivermectin efficacy anyway.”
So, was this the definitive answer proclaimed by mainstream sources? Nass thinks otherwise:
“I would say that instead, it was a failed trial due to the 391 placebo recipients who admitted they did not follow protocol versus the 55 in the ivermectin arm.”
More questions than answers
Rather than pounding the final nail in the coffin around ivermectin’s utility in treating COVID, the NEJM study raises more questions.
- What would the effect have been if a higher dose shown to be effective were administered?
- What would be the benefit of this medicine in patients with no risk factors?
- How statistically significant would the results have been if more participants were enrolled?
- Why weren’t more participants enrolled as the study progressed given the emerging benefit of the drug and the absence of adverse events?
- Why did the investigators define a primary outcome with such different real-world implications (ER visits vs hospitalizations)?
- With less than 50% of the placebo arm adhering to the study protocol, why were their outcomes included in the analysis?
- What effect did vaccination status have on outcome? If this is the primary means endorsed to prevent hospitalization, why wasn’t vaccination status mentioned as a confounder?
- Did the investigators choose to limit the study as it became clear that an Ivermectin benefit would be too big to ignore?
Given these obvious issues with the study, it is becoming even more clear where the real story is: Neither The Wall Street Journal or The New York Times are willing to pursue startling details around how corporate interests are corrupting scientific opinion as reported here.
Instead, these iconic journals chose to report on a scientific study on or prior to the day of publication using misleading headlines backed up by flimsy investigations conducted by journalists with no capacity to dissect the analysis or data.
Here’s a bigger question: Are they incompetent, or complicit, too?
The corrupt establishment will do anything to suppress sites like the Burning Platform from revealing the truth. The corporate media does this by demonetizing sites like mine by blackballing the site from advertising revenue. If you get value from this site, please keep it running with a donation. [Burning Platform LLC – PO Box 1520 Kulpsville, PA 19443] or Paypal
