Statistical analysis shows that NOBODY under 60 should take the COVID vaccine
Guest Post by Steve Kirsch
This is a PRELIMINARY result based on over 1,500 death reports we’ve received so far. You are welcome to download our data yourself and analyze it and see if you agree. You may find some new things.
Summary
This is big. Really big. This may prove to be one of the most important articles I will write this year.
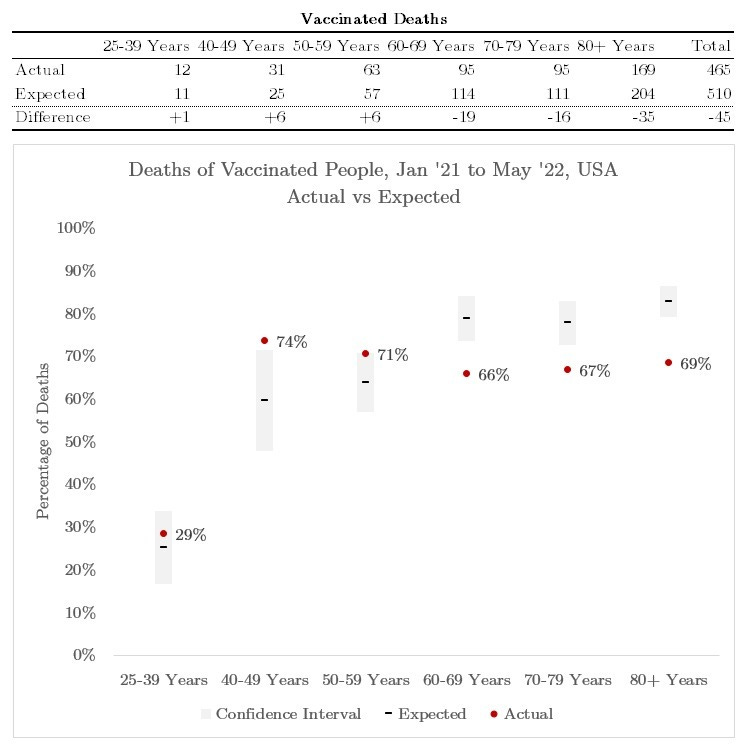
Figure 1 below is an analysis of survey data I collected. The analysis shows that the vaccines are harmful to those under 60. The red dots higher than the error bar means more vaccinated people observed dead than expected based on the population of vaccinated to all people. In other words, if we vaccinated 60% of people (middle of the grey bar) and 70% (red dot) of the deaths are vaccinated, we have a serious problem.
The precautionary principle of medicine suggests if you are under 60 and thinking of taking a vaccine, you shouldn’t. These preliminary results are both statistically significant.
However, there could be errors in the analysis and/or survey bias errors that will change the result, so this is preliminary. I hope to make these not preliminary in a few days.
I created a mortality survey which asked people to report the date, age, and vaccine status of the people who died who they had the tightest relationship with. You could report as many deaths as you wanted for people you PERSONALLY knew, but if you didn’t report them all, start with the person closest to you. All deaths should be reported no matter what the cause of the death. If they died after December 1, 2020, report it.
The first 1,700+ results are in and Joel Smalley had time to do the analysis. It is stunning. The conclusion is very clear: nobody under 60 years old should get the vaccine because there is no evidence of a benefit. In fact, if you are between 40-60, it’s clear that vaccination makes it more likely you’ll die, not less likely. It’s statistically significant. The result that the younger you are, the less sense it makes, is consistent with what pretty much everyone has been saying.
The only thing that surprised me in the analysis is that data showed that if you are 60 and older, getting vaccinated reduces your chance of dying.
I’m astonished by the data showing a benefit for >60 because it is inconsistent with the VAERS data (which is off the charts showing nearly 500,000 deaths), embalmer data, and this article about 6 elderly deaths in Palo Alto out of 9 people vaccinated, and medicare data, and UK ONS data. I’m confident of the embalmer data and Palo Alto deaths: there is absolutely no way if the vaccine was protective that those events could occur. This means there must be an error in the analysis or confounding of the data. There cannot be two truths.
My advice is to avoid the COVID vaccines for ALL ages. If you get sick, get early treatment. This is because we have strong DIRECT evidence (embalmer, nursing home data is clearly strongly negative) that the vaccines are deadly to the elderly and until someone explains how the direct evidence is wrong, the precautionary rule of medicine says we should respect that possibility and thus early treatment is the preferred alternative.
In other words, if you have conflicting evidence, better to avoid that option until the conflict is resolved especially when the more direct evidence suggests that the intervention is deadly.
I’m not trying to cherry pick here. I’m saying that quality direct evidence rules over calculated numbers. If the best evidence I have is calculated numbers, I go with that.
For example, if the calculations show that the vaccine is safe for those over 60 and I find that 9 out of 10 people over 60 who get the shot die within 24 hours from blood clots, which evidence do you believe?
I cannot reconcile the discrepancy at this time.
Joel may have made a mistake. So take all these results (including under 60) with a grain of salt for now. We are getting close to finding the truth. There could be a bias that shifts everything in one direction. We’ll see.
We want to have many eyes on this data before we will announce a definitive result.
I’m making all the data to date available for people to validate or invalidate the result. I’ll periodically update the spreadsheet as we collect more data.
We’ll be collecting a lot more data to refine the result and employ 3 different third party survey firms as well. This eliminates the risk of people trying to game the survey (not that anyone would do that). So if the independent polling firm results don’t match our results, we’ll look for what happened. Using five or more sources of independent data (mine, Joe’s, 3 polling firms, etc.) will give everyone more confidence that the results are valid.
Note that the definition of vaccinated here is “got the vaccine” not “two weeks after they got the vaccine.” We are NOT using public data that is encumbered this way. Such definitions are misleading since if the vaccine kills everyone within two weeks of the shot, the vaccines look amazingly safe and not being vaccinated looks risky.
Notes on Figure 1 from Joel Smalley
Joel Smalley did the analysis of the two datasets described below.
Figure 1 represents the percentage of deaths between Jan ’21 and May ’22 that were of vaccinated people of different age groups compared to the expected percentage of deaths.
The expected percentage was determined as a function of the vaccinated population on the day of death of a vaccinated or unvaccinated person in the dataset.
The expected value was calculated by randomly selecting a number from 1 to 100 and specifying it as vaccinated if it was at or below the vaccinated population for that age range on that day. Otherwise, it would be considered an unvaccinated death.
The model was run 1,000 times and the average point estimate taken to be the expected value with a confidence interval of 2 standard deviations from the mean.
The survey
There were two versions of the survey.
The first one left too much wiggle room in the responses so the first 931 results need to be scrubbed to put in a consistent format to be usable. I modified the survey mid-survey so that messes things up a bit; that column needs to be normalized.
If someone would like to volunteer to do that, please note that in the comments and then email me the updated spreadsheet at stevekirsch-request (at) protonmail.com. That email is NOT monitored by me and if you send anything there other than in response to a specific request it will be ignored.
The data
PostVaxMortality1: 932 rows. Note that I changed things around mid survey, so be careful. This is the database I need someone to clean up and I’ll replace it, e.g., “Days after dose” column was changed from fill in to choose 1. However, most of the other columns are fine so you can use them immediately. Just check the column first.
PostVaxMortality2: 834 rows. No need to fix the data. Use immediately
Technical logistics
- It took me about an hour to design the survey questions and about 25 minutes to create the Google form
- It took me about 20 minutes to write up a promo on substack and launch the survey
- It took 24 hours to get over 1,000 responses
- It took Joel 30 minutes to analyze the results
That’s damn time efficient. Can’t imagine why the CDC can’t replicate this?
Limitations
- Most of the respondents were my followers so can be classified as “anti-vaxx.” However, this survey makes the case that the vaccines work for those over 60. If it was biased that people were only reporting people with vaccines who died right after, this signal would be impossible. So it’s unlikely there is selection bias, but there could be. That’s why we are using 3 outside survey firms for our next data collection.
- Joel did the analysis very quickly and may not have adjusted for all the biases and confounders that are always present.
- Nobody else has had a chance yet to replicate or refute the result on the data collected so far.
- Things to consider that could affect the final result include: the virus IFR changes over time, the age mix of people in the vaccinated group changes, background death rates are seasonal and differ in each age range, people may report someone who dies 13 days after Dose 1 to be unvaccinated, people who answer the survey.
- For the purposes of this survey, only the date, age at death, and vaccination status of the deceased matter. These can be misreported.
- There may be an error in the analysis.
- There may be errors in the public underlying data such as reporting vaccination status as vaccinated 14 days after the jab rather than at the moment of the jab.
- This is not a complete list.
In short, we’re getting very close to the truth.
Was my sample biased?
The survey data we use is objective, fact-based questions: date, age, got vax?
The results we got show the younger you are, the harder to justify the vaccines are. This shouldn’t surprise anyone.
People don’t get to chose who dies. But they could have selective recall.
However the results were consistent with other research.
In her interview with Freddie Sayers, Professor Christine Stabell Benn said her best guess on current data is that those under 50 probably don’t benefit from the vaccine. She has been looking at non-specific effects of vaccines and finds the mRNA vaccines may have been associated with an overall higher mortality from non-covid related issues.
What will happen next
One of two things will happen now:
- The medical community will do their own survey and replicate the result and realize they’ve been had. They will call a halt to the vaccine immediately for those under 60.
- The medical community will fail to replicate the result and call me a misinformation spreader. However, this will only cause them to dig themselves even deeper into a hole because they know other independent people will be able to replicate it. There will not be a rock big enough for them to hide under.
Will the medical community double down in the face of evidence they cannot refute? Or admit they made the biggest error of all time?
Finally, it is ridiculous that nobody in the world has done a similar survey and published the results. Nothing prevented anyone from doing this. The only person that I’m aware of doing this is UCSF Professor Aditi Bhargava. I’m a major funder of her work.
Anyone could have done the same survey I did. It took only an hour or so to create the survey the first time and I had 1,000 results back less than 24 hours later. Why is the CDC incapable of doing this?
Why isn’t there a proper risk benefit analysis of these vaccines from the CDC? We have NOTHING.
Nobody in the medical community demanded evidence of a positive risk-benefit. You can’t assume that the vaccines are safe. That would be trusting a drug company who has stated, without any evidence whatsoever, that all the excess deaths in the vaccine group were not related to the vaccine. The FDA and medical community accept their word without asking for proof.
Nobody wanted to see the risk benefit analysis. Did you ever hear the VRBPAC or ACIP committee members asking for one? Of course not!!
So I did it using the VAERS data and the UK ONS data and here’s what I found:
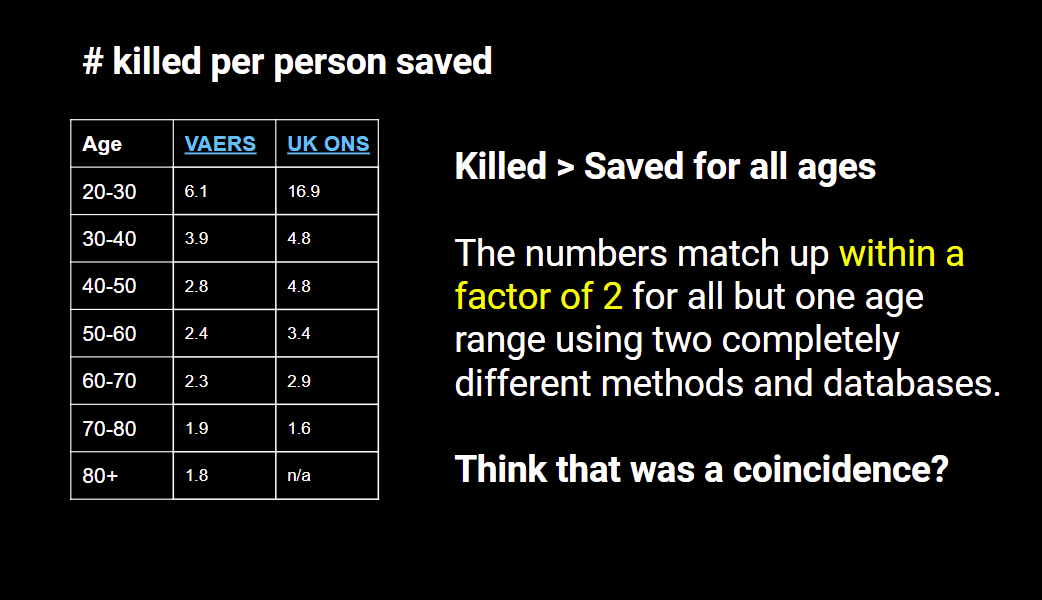
If I got it wrong, where is the CORRECT analysis of that same data? People like to throw darts at my work, but they NEVER show me the CORRECT analysis of the same data set. I wonder why that is? Some claim the VAERS data is “unreliable” but that’s a lame excuse for not looking at. Nothing keeps you from doing a proper analysis and then having a Limitations section that notices that VAERS is underreported.
Why isn’t there a study that follows 100,000 unvaccinated people over time vs. 100,000 vaccinated in equally matched groups and observing how many people are alive after each week in the two groups and categorize each death as COVID or not. You’d look at the benefit (decrease in # of COVID deaths compared to the unvaccinated group) and risk (increase in non-COVID all-cause mortality in the vaccinated group) and compute the ratio. That gives you a risk benefit analysis stratified by age and you can see how the risk/benefit changes over time so people can answer the question, “If I am age xxx, does it make sense for me to be vaccinated today?”
Nobody has asked for this. Why? Do we not want to know?
Any sane society should be DEMANDING such an analysis before even considering approving such a drug. Mandating a drug with no risk benefit analysis that is obviously not being done is the height of irresponsibility.
Why is nobody speaking out about this?
Why is it so unreasonable to ask for a risk-benefit analysis BEFORE doctors advise their patients? There is simply no excuse for not computing this from this “real world” mass experiment.
If we don’t have the data, we need to get it before we experiment on people.
We need to stop the experiment now.
Is it the responsibility of electrical engineers to check the work of the medical community?
That this survey and analysis comes from a high tech software executive in Silicon Valley with two EECS degrees from MIT is an embarrassment. This is not my responsibility to do this. I did it because nobody in the government, medical community, no public health official, and nobody in the mainstream media did it. It’s almost as if they didn’t want to know that the vaccine worked or not.
If the vaccines aren’t protective, what can we do? Early treatment!
Just like Dorothy could have always returned to Kansas just by clicking her slippers, we have had the cheapest, safest, and fastest solution to treat COVID available since March 2020.
Early treatment such as the Fareed-Tyson protocol has a near perfect track record against COVID with few hospitalizations and no deaths. The NIH and mainstream doctors (who follow whatever the NIH says) ignore it. That tells you everything.
So what we should be telling people is have the drugs on-hand so you can start treatment ASAP after you get sick.
Instead, the CDC tells people to get vaccinated and that early treatment with repurposed drugs should be ignored.
We’d be better off if everyone listened carefully to what the CDC says and does the opposite. I’m serious. I can’t think of anything they’ve recommended that has been helpful in the pandemic. I’d love to debate them on that. I could sell tickets to that one.
We never needed screening, lockdowns, social distancing, remdesivir, masks, vaccines, etc. All we needed is one thing: let people know early treatment works if given early.
How you can help
- If you are into data analysis, have a look at the data (see “The data” section above)
- If you live in the UK, please take Joel’s survey of deaths in the UK so we can compare the results.
- If you live anywhere else, please take my survey if you have not already
Summary
We now have a simple objective way to assess the safety and efficacy of a vaccine. Anyone can do the surveys themselves to verify the result. Anyone can take our data and analyze it.
The analysis is troubling: nobody under 60 should take the vaccine.
I’m awaiting confirmation from other researchers.
Please share this article so we can collect more data to reduce the size of the error bars. If you are not a subscriber, please subscribe so we can let you know what the subsequent analysis shows.
With your help, we can change the world. Thank you!
The corrupt establishment will do anything to suppress sites like the Burning Platform from revealing the truth. The corporate media does this by demonetizing sites like mine by blackballing the site from advertising revenue. If you get value from this site, please keep it running with a donation. [Burning Platform LLC – PO Box 1520 Kulpsville, PA 19443] or Paypal
—————————————————–
Use promo code ILMF2, and save up to 66% on all MyPillow purchases. (The Burning Platform benefits when you use this promo code.)



