How CDC Blatantly Uses Weekly Reports to Spread COVID Disinformation: Three Examples
The authors of the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report are afforded the luxury of broadcasting their findings to massive audiences through media outlets that don’t hold them accountable for even gross lapses in scientific rigor.

The Centers for Disease Control and Prevention (CDC) — the primary U.S. health protection agency — publicly pledges, among other things, to “base all public health decisions on the highest quality scientific data that is derived openly and objectively.”
The CDC’s “primary vehicle for scientific publication of timely, reliable, authoritative, accurate, objective, and useful public health information and recommendations,” according to the agency, is its Morbidity and Mortality Weekly Report (MMWR).
The CDC states that the MMWR readership consists predominantly of physicians, nurses, public health practitioners, epidemiologists and other scientists, researchers, educators and laboratorians.
However, these weekly reports also serve as the means by which the agency disseminates its scientific findings to a much wider readership through media outlets that inform hundreds of millions of people.
Though the CDC asserts its MMWRs reliably communicate accurate and objective public health information, the reports are not subject to peer review, and the data behind the scientific findings are not always available to the public.
Moreover, when the media summarizes MMWR findings in articles intended for the general public, they often omit or misrepresent important details.
As a result, the reports often steer public opinion to a level of certainty the authors of the reports themselves cannot justify — and often, to incorrect conclusions.
As Marty Makary M.D., M.P.H., and Tracy Beth Høeg M.D., Ph.D., recently revealed, some officials within the CDC claim the heads of their agencies “are using weak or flawed data to make critically important public health decisions, that such decisions are being driven by what’s politically palatable to people in Washington or to the Biden administration and that they have a myopic focus on one virus instead of overall health.”
In this article, I will demonstrate how the CDC used three key MMWRs to compel the public to comply with pandemic response measures.
These reports were flawed to an extent suggesting more than mere incompetence or even negligence — they were deliberate attempts by CDC scientists to mislead the public.
These MMWRs address the effectiveness of mask mandates (March 5, 2021), vaccine safety during pregnancy (Jan. 7, 2022) and the risk of COVID-19 in children (April 22, 2022).
Do I need to wear a mask?
The New York Times in May ran this story, “Why Masks work, but Mandates Haven’t,” in which the author concluded:
“When you look at the data on mask-wearing — both before vaccines were available and after, as well as both in the U.S. and abroad — you struggle to see any patterns.”
But that’s not what the CDC concluded in its March 5, 2021, MMWR:
“Mask mandates were associated with statistically significant decreases in county-level daily COVID-19 case and death growth rates within 20 days of implementation.”
How could the CDC claim there was a statistically significant decrease in cases within 20 days of mask mandate implementation if there were no patterns in the data?
The explanation is necessarily detailed because the CDC authors’ methodology is so devious. A detailed critique of the agency’s approach is offered in this preprint paper (Mittledorf, Setty) which I will summarize here.
The CDC researchers examined the number of COVID-19 cases reported each day in each U.S. county that implemented a mask mandate.
Then they calculated the Daily Growth Rate (DGR) of cases (and deaths) in each county on each day for 60 days preceding the countywide mandate and for 100 days afterward.
The authors purportedly showed the DGR fell after mandates were imposed. It is important to realize that when the DGR falls on a certain day, it does not mean that fewer new cases occurred on that day compared to the day before — it means the number of new cases is not growing as fast as it was prior to that day.
In other words, by using DGR as the measure of interest, the authors can still claim a “significant decrease in COVID-19 case growth rate” even if the number of new cases on a given day is larger than the day before.
When data for 2,313 U.S. counties were tallied into a composite graph, this is what they found:
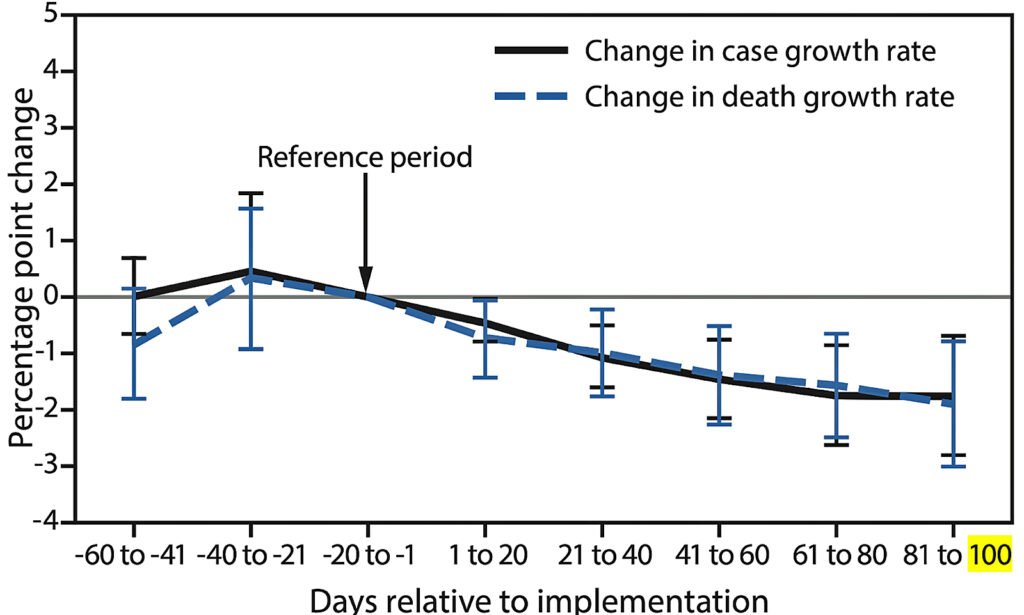
Note that mandates were implemented at different times in different counties, so the “reference period” occurred at different times during the year depending on the county.
Furthermore, the plot indicates the DGR at different times relative to the DGR at the reference period.
In other words, when the plot falls below zero it does not mean the DGR is negative — it means it was less than it was during the 20 days prior to the institution of the mandate (the “reference period”).
Nevertheless, it seems that on average, the DGR falls after the implementation of mask mandates.
However, what was happening prior to the reference period?
We don’t know — and neither do the authors of the CDC report.
Figure 1 includes ranges of confidence intervals that stretch above and below that of the reference period prior to mask mandate implementation. Because the upper bound of the DGR is greater than the reference period prior to the point mandates were implemented, it is entirely possible the DGR was already in decline prior to the implementation of mask mandates.
The authors’ own data and calculations demonstrate the drop in DGR may have had nothing to do with mask mandates at all.
In other words, the authors also could have concluded mask mandates were associated with a drop in the DGR 40 days prior to their implementation.
In fact, this is clearly demonstrated in the graph. The DGR for both cases and deaths is highest in the period 20 to 40 days before the mandate.
How amazing! Masks seem to work several weeks before people are forced to wear them!
Beyond ignoring what their own data suggested, the CDC authors made two very suspicious decisions when designing their study.
The CDC chose to limit its analysis to 100 days after mandates were instituted. Was this an arbitrary length of time? Or was there another reason?
We examined data from the entire country for the period of the study and plotted the DGR for a full year here:
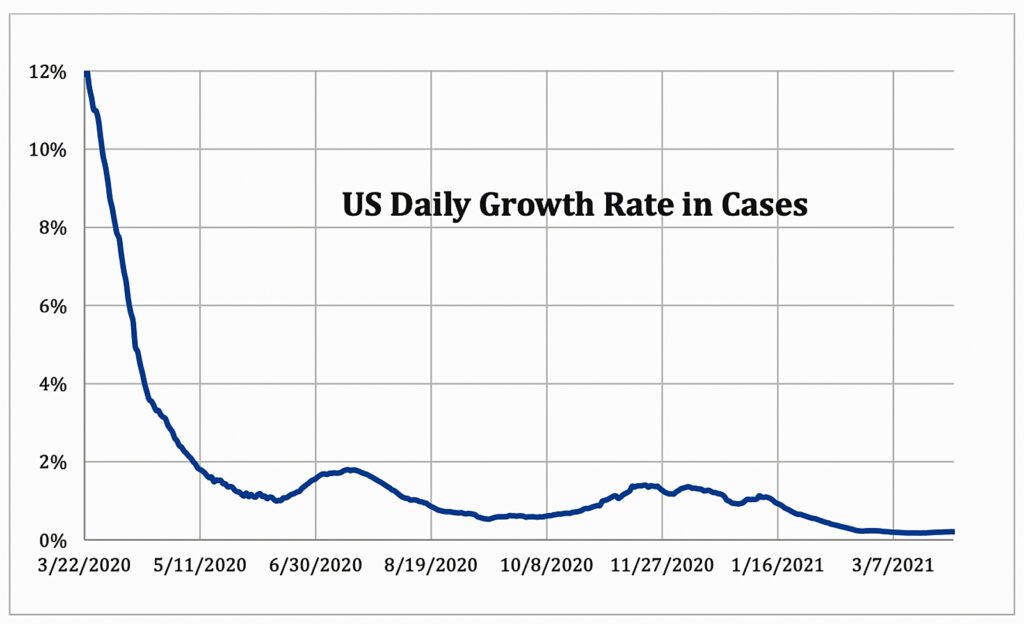
Figure 2 clearly demonstrates the DGR was already in steep decline at the beginning of the study period, just as pointed out earlier.
The graph also indicates the DGR temporarily rose at the beginning of the summer, then fell, then began to rise again at the beginning of the autumn.
Because the overwhelming majority of mask mandates began in the late spring and early summer, a 100-day window of analysis will show a declining DGR because it will miss the increase in DGR in the fall.
Also note that a shorter period of observation, say 50 days, would have resulted in equivocal or opposite findings as the summer “bump” would have made it seem like mask mandates had no effect or possibly increased the DGR.
The CDC conveniently chose an observational window that could be neatly nestled between the periods of higher DGR.
For example, the state of California imposed statewide mandates on June 18, 2020. Using CDC data, this is what a plot of the DGR for the state looks like if the period of observation were extended beyond 100 days:

The DGR at the end of the 100 days (Sept. 25, 2020) was approximately 0.5%, or about 1.5% lower than it was prior to the mandates in that state. However, two months later, the DGR had returned to its pre-mandate level.
If the CDC extended its window of analysis it would not have been able to claim there was any benefit from the mask mandates. The pattern was similar in the country as a whole, as demonstrated in Figure 2.
Did the CDC just get lucky with its window of observation? Or was the agency seeking a way to justify unpopular masking policies that had been in effect for nearly a year at the time this study was released?
At this point, any reasonable researcher would suspect the CDC’s authors were engaged in elaborate hand-waving to lead the public to a predetermined conclusion.
How can we know for sure?
If the CDC were truly interested in demonstrating a fall in the DGR due to mask mandates, the authors of the study would have asked the most basic of questions: What happened in counties that did NOT institute mask mandates during the study period? In other words, what happened in the “control” group during the same time?
Though there were 829 U.S. counties that did not implement mask mandates, the CDC researchers did not analyze any of them to test their hypothesis. Why didn’t they?
We did. From our preprint study linked above, this is what we found:
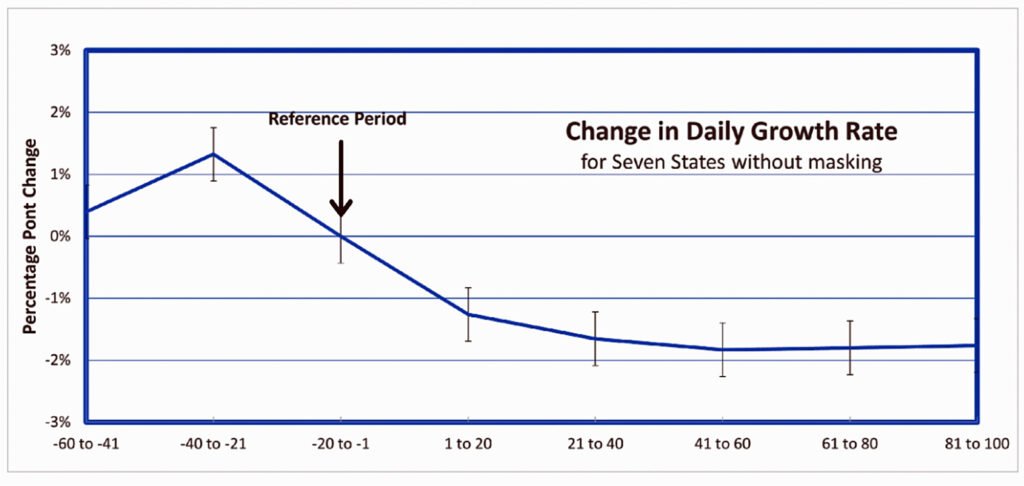
Using publicly available data from the CDC and an arbitrary “reference period” of Aug. 6, 2020 (roughly in the middle of the CDC’s study period date), we calculated the DGR in counties of seven states without mandates also fell to similar levels at the end of 100 days.
In other words, the decrease in DGR had nothing to do with the imposition of mask mandates. It was due to a predictable pattern of any infectious disease as it spreads through a population over time — whether or not people were forced to wear masks.
This would have been obvious if the CDC were actually interested in being scientific.
Nevertheless, the New York Times unhesitatingly covered the CDC’s findings on the very same day the MMWR was released in this article: “The Virus Spread Where Restaurants Reopened or Mask Mandates Were Absent.”
The Times quoted CDC Director Dr. Rochelle Walensky who said, “You have decreases in cases and deaths when you wear masks,” and Joseph Allen, an associate professor at Harvard’s T.H. Chan School of Public Health, who said;
“The study is not surprising. What’s surprising is that we see some states ignoring all of the evidence and opening up quickly, and removing mask mandates.”
The Times wasn’t the only media outlet to report on the flawed study.
CNBC posted this article: “CDC study finds easing mask and restaurant rules led to more Covid cases and deaths, as some states move to lift restrictions.”
And U.S. News and World Report ran an article under this headline: “Mask Use Associated With Decline in Coronavirus Cases, Deaths, CDC Says.”
In fact, more than 100 media outlets cited the CDC study within 24 hours of its release — but not one questioned the authors’ analysis.
In their defense, that is not their job. The media’s role is to simply relay what the CDC has to say. Yet without any oversight or accountability, the CDC can conclude whatever it chooses.
Because the mainstream media machine grants the CDC infallible status, the public is lured into an illusion that “the science is settled.”
But why would the CDC authors go to such lengths to manufacture an unfounded position on mask mandates? Surely they realized their methodology would be scrutinized and found to be manipulative by those who don’t consider the agency to be irreproachable. Why risk their credibility? What do they have to gain?
The MMWR was released on a Friday. On the following Monday, March 8, 2021, the CDC tells us, as NBC News reported:
“‘As more Americans are vaccinated, a growing body of evidence now tells us that there are some activities fully vaccinated people can do,’ the CDC’s director, Dr. Rochelle Walensky said during a White House Covid-19 briefing Monday.
“‘The latest science [emphasis added],’ Walensky said, ‘suggests that fully vaccinated people can congregate indoors with other fully vaccinated people without wearing face coverings or practicing physical distancing.’”
And there you have it.
Three days after the flawed MMWR was released, being with other human beings indoors without masks became a privilege reserved exclusively for the “fully vaccinated.”
The “latest science” must demonstrate that masks offer some protection, however miniscule. If there were no benefit to mask wearing, there would be one less carrot authorities could use to get the public to comply with their vaccine agenda.
Are COVID-19 vaccines safe during pregnancy?
In a Jan. 7 MMWR, the authors addressed another important public concern: Are the vaccines safe during pregnancy?
To answer this question, CDC authors examined the incidence of only two pregnancy outcomes: preterm births and small-for-gestational age (SGA) in unvaccinated and vaccinated mothers.
They concluded:
“CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant (including those who are lactating), who are trying to become pregnant now, or who might become pregnant in the future to reduce the risk for severe COVID-19–associated outcomes.”
Their assurances came more than a year after the first COVID-19 vaccine was granted Emergency Use Authorization, in December 2020.
In this example, CDC authors did not have to cherry-pick periods of observation or ignore control groups to make their “conclusions.”
Here, they relied on comparing two poorly matched groups of mothers (the unvaccinated were at a higher risk of pregnancy complications):
- There were greater than 50% more mothers in the unvaccinated group classified as having inadequate prenatal care than in the vaccinated group.
- Obesity, a risk for preterm birth, was also overrepresented in the unvaccinated group (29% vs 23.9%) compared to the vaccinated.
- There were greater than three times more African American women in the unvaccinated group than in the vaccinated group. The CDC acknowledges African American mothers may have as much as a 50% greater risk for preterm birth compared to white mothers.
- COVID-19 infection, another potentially important confounder, was present in the unvaccinated group at a 25% greater incidence than in the vaccinated cohort. Viral infections early in pregnancy are particularly deleterious to the developing fetus.
The differences between the two cohorts should have been obvious to the authors. Why?
Because they found the risk of preterm birth and SGA in the vaccinated weren’t equal to that in the unvaccinated group — in fact, they were lower (adjusted Hazard Ratios were 0.91 and 0.95 respectively).
These numbers were very close to being statistically significant.
Amazing. Masks prevent the spread of the disease weeks before they are mandated and now we find that the COVID-19 jabs aren’t just safe, they can actually lower the risk of preterm birth and SGA!
Why didn’t the authors report that their data indicated that COVID-19 vaccines somehow reduce the risk of these outcomes? Was it because the data weren’t quite statistically significant?
Or was it because they didn’t want to draw attention to the fact that the unvaccinated group was at higher risk for these outcomes to begin with?
But the most glaring deficit in the CDC analysis was the scarcity of vaccinated mothers who received a vaccine in the first trimester in this study.
The risk of untoward outcomes (birth defects, miscarriages) in pregnancy is greatest during the first third of pregnancy, a time when crucial embryonic structures are developing.
This is the period of time where maternal health is particularly important and exposure to toxins, infections and certain medicines must be minimized or eliminated entirely if possible.
Only 172 of more than 10,000 (1.7%) vaccinated mothers in the study received a vaccine in the first trimester.
This was acknowledged by the authors who explicitly stated: “Because of the small number of first-trimester exposures, aHRs (adjusted Hazard Ratios) for first-trimester vaccination could not be calculated.”
If they could not calculate the risk of the vaccine in the first trimester, on what basis could they assure the recently pregnant, those who are trying to become pregnant and those who might become pregnant in the future that this experimental intervention was safe?
They couldn’t — but they did anyway. And once again, mainstream media outlets wasted little time in spreading the “good news”:
- Boston.com (Jan. 18, 2022): “New study bolsters case for COVID vaccination during pregnancy.”
- Medical News Today (Jan. 11, 2022): “COVID-19 vaccination during pregnancy not linked to adverse birth outcomes.”
- Medscape (Jan. 12, 2022): “COVID-19 Vaccination During Pregnancy Not Linked to Complications at Birth: US Study.”
And even on other continents:
- Juta Medical Brief, Africa’s Medical Media Digest (Jan. 12, 2022): “COVID vaccination not linked to premature birth or unusually small babies — CDC study.”
- newKerala.com (Jan. 8, 2022): “Researchers say COVID-19 vaccine does not disrupt pregnancy.”
Even People magazine, a go-to source for the latest in medical research and public health, helped spread the CDC gospel: “COVID Vaccines Among Pregnant Women Are Not Linked to Pre-Term Births, According to New Study.”
Should I vaccinate my child?
In this April 19 MMWR, CDC authors compared the risk of hospitalization of 5- to 11-year-old children from COVID-19 during three different time periods: pre-Delta, Delta and Omicron.
By the end of the period of observation, Feb. 28, 2022, only approximately 30% of children in this age group had received both doses of the primary series of COVID-19 vaccines. The experimental product had been authorized for these children four months prior.
Was this report a “reliable, accurate and objective” publication of available data? Or was it an attempt to persuade parents to inoculate their children by making contradictory statements and illogical reasoning?
Read on and decide for yourself.
The April 19 report uses a different set of tactics to lead the unwary reader to false conclusions. In this example, statements are made in the text of the paper that are true, but also irrelevant or misleading.
From the CDC’s own data (Table 1), among hospitalized children aged 5-11 who had laboratory-confirmed COVID-19, more were admitted because of COVID-19 during the Delta wave (364) than during the Omicron wave (160). These numbers were statistically significant.
Yet the authors did not mention this fact in their discussion. Instead, they chose to compare the rate of hospitalization during a single, one-week peak of each wave: 2.8 per 100,000 during Omicron, and 1.2 per 100,000 during Delta.
Clearly, it is the total number of hospitalizations that is salient when assessing the risk of the predominant variant in circulation — not the number during a brief period of each wave.
Intentionally or not, the authors suggested Omicron is even more dangerous than Delta — which is not true.
This same strategy was used in yet another MMWR (from March 15, 2022) that sought to convince parents of children under age 5 to inoculate their young children by comparing hospitalizations at the peak of each wave rather than the total number of hospitalizations.
Dr. Meryl Nass dissects that CDC report here.
What are parents to do if they believe Omicron is more dangerous than the Delta variant? The answer is apparently obvious.
The authors of the April 19 MMWR extracted hospitalization rates from 14 states for fully vaccinated and unvaccinated children in this age group: Unvaccinated kids are 2.1 times more likely to be hospitalized than those who were fully vaccinated.
Surely this should be enough to motivate the uncertain parent. However, when there is a potential risk it is imperative to assess the absolute risk of the intervention, not just the relative benefit.
In this case, the risk of hospitalization during the Omicron wave was 19.1 per 100,000 in the unvaccinated compared to 9.2 per 100,000 in the fully jabbed.
This means roughly 10,000 children had to be fully vaccinated to prevent a single hospitalization — a striking number the CDC authors did not mention.
In typical fashion, the CDC authors don’t mention the risk, which is yet to be established, of the experimental vaccine.
Though the authors accurately reported on the aggregate data, they mysteriously chose to include another statistic: 87% of hospitalized children were unvaccinated.
How could roughly 7 of 8 hospitalized kids (87%) be unvaccinated if the rate of hospitalization was only about double in the unjabbed?
The answer is that most children (70% or more) hadn’t been inoculated during this time. Why would they mention this true-but-misleading statistic?
We can’t know with any certainty, but it certainly makes a good talking point.
Forbes did not consider such questions when it ran this piece the same day: “87% Of Kids Hospitalized With Covid During Omicron Wave Were Unvaccinated, CDC Says.”
Other media outlets also fell into line and ran stories with misleading headlines based on this MMWR:
- The World Business News: “Omicron Was More Severe for Unvaccinated Children in 5-to-11 Age Group, Study Shows.”
- Axios: “CDC: 87% of children hospitalized during U.S. Omicron surge unvaccinated.”
- BNN Bloomberg ran this: “Unvaccinated Kids Bore Brunt of Omicron Wave, CDC Report Says.” The title is not inaccurate. However, the very first line of the story predictably reads: “Almost 90% of U.S. children hospitalized for Covid during the omicron wave this winter were unvaccinated, according to a government study.”
If you read these articles you will find they all regurgitate the same misleading statements the CDC authors included in the text of their report.
On this page, there are dozens of articles titled (more or less) “Unvaccinated Children Hospitalized at Twice the Rate During Omicron Surge: US Study.” All cite the misleading MMWR.
The data that supported the fact that the unvaccinated children were twice as likely to be hospitalized was found here on the CDC website. The data from the MMWR study period has since been updated.
This is what the numbers now show:
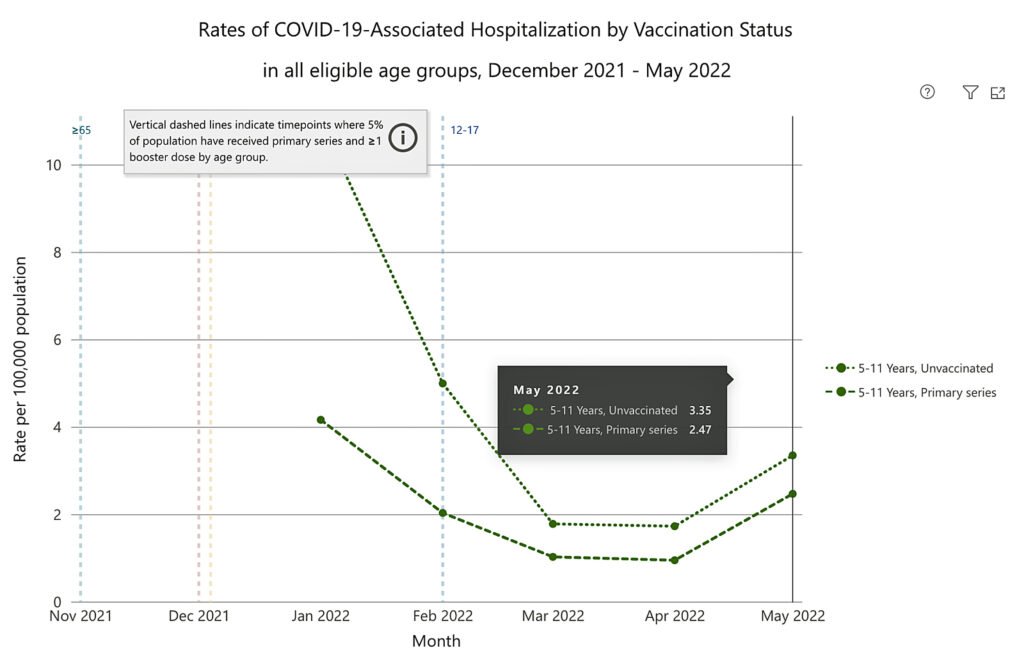
As of May 2022, in the 5-to-11 age group, there is a difference of 0.88 hospitalizations (3.35 – 2.47) per month in every 100,000 kids between the unvaccinated and vaccinated.
This means more than 113,000 children in that age group must receive both doses to prevent a single hospitalization per month.
In yet a final attempt to confuse the reader, the CDC authors state up front in their highlighted “Summary”:
“Increasing COVID-19 vaccination coverage among children aged 5–11 years, particularly among racial and ethnic minority groups disproportionately affected by COVID-19, can prevent COVID-19–associated hospitalization and severe outcomes.”
Read that statement closely. They clearly state that increasing vaccination coverage in this age group can prevent severe outcomes.
Can they prevent severe outcomes? Maybe. But did they? Not according to their data.
The authors later correct themselves in the body of the report: “There were no significant differences for severe outcomes by vaccination status.”
Which statement do you think the media outlets chose to publish?
No limits to their treachery . . .
The CDC website describes its MMWR series here:
“Often called ‘the voice of CDC,’ the MMWR series is the agency’s primary vehicle for scientific publication of timely, reliable, authoritative, accurate, objective, and useful public health information and recommendations.”
If the MMWR series is “the voice of CDC,” mainstream media serves as its mouthpiece.
By working together, the CDC authors are afforded the luxury of broadcasting their findings to massive audiences through media outlets that will not — and in many cases cannot — hold them accountable for even gross lapses in scientific rigor.
In my opinion, these examples demonstrate something more than honest mistakes. These are egregious misrepresentations of data that were meant to deliberately mislead the public, public officials and the medical establishment in order to galvanize support around unpopular mandates and push the “safe and effective” narrative.
There wasn’t a “statistically significant decrease in COVID-19 case counts associated with mask mandates.”
There wasn’t enough data to recommend the COVID-19 vaccine for mothers who recently became pregnant.
The data did not demonstrate that the COVID-19 vaccine can prevent severe outcomes in children ages 5 to 11.
The common thread in all three of these cases is that an uninformed reader of these reports will readily conclude that getting the jab is the best way to return to normalcy or protect a young child or a pregnancy.
We can speculate that Big Pharma’s insatiable thirst for profit is behind the CDC and corporate media, but with tens of billions of dollars already earned, why are they so desperate to keep the misinformation campaign going?

The most obvious answer is that they cannot afford not to. From the initial adult vaccine trials conducted in the summer and fall of 2020 to the most recent trials in the pediatric population, all placebo recipients were given the jab after just a few short months.
This resulted in only short-term efficacy and safety data. Using trial outcomes alone, no long-term safety assessments can be made. If there is a significant risk in the middle to long term, it can be estimated only through observational studies in the population.
The unvaccinated millions and their enduring health will stand as the biggest threat to the industry’s income stream and our health authorities’ credibility.
Authors of the CDC MMWR series are not accountable to anyone, including the CDC director who parrots their findings, or the public who rely on captured media outlets to ask the right questions.
With this level of impunity, there are no limits to their treachery.
Image credit for Figures 2-4: Josh Mitteldorf and Madhava Setty.
The corrupt establishment will do anything to suppress sites like the Burning Platform from revealing the truth. The corporate media does this by demonetizing sites like mine by blackballing the site from advertising revenue. If you get value from this site, please keep it running with a donation. [Burning Platform LLC – PO Box 1520 Kulpsville, PA 19443] or Paypal
—————————————————–
Use promo code ILMF2, and save up to 66% on all MyPillow purchases. (The Burning Platform benefits when you use this promo code.)

