The Bivalent Booster Disaster
Guest Post by Rav Aurora
Over the past four months, the White House, Centers for Disease Control and Prevention (CDC), and Food and Drug Administration (FDA) have vigorously pushed the new bivalent vaccine on all eligible Americans. In his final White House briefing, Dr. Anthony Fauci stated, “Please, for your own safety, for that of your family, get your updated COVID-19 shot as soon as you’re eligible to protect yourself, your family, and your community.”
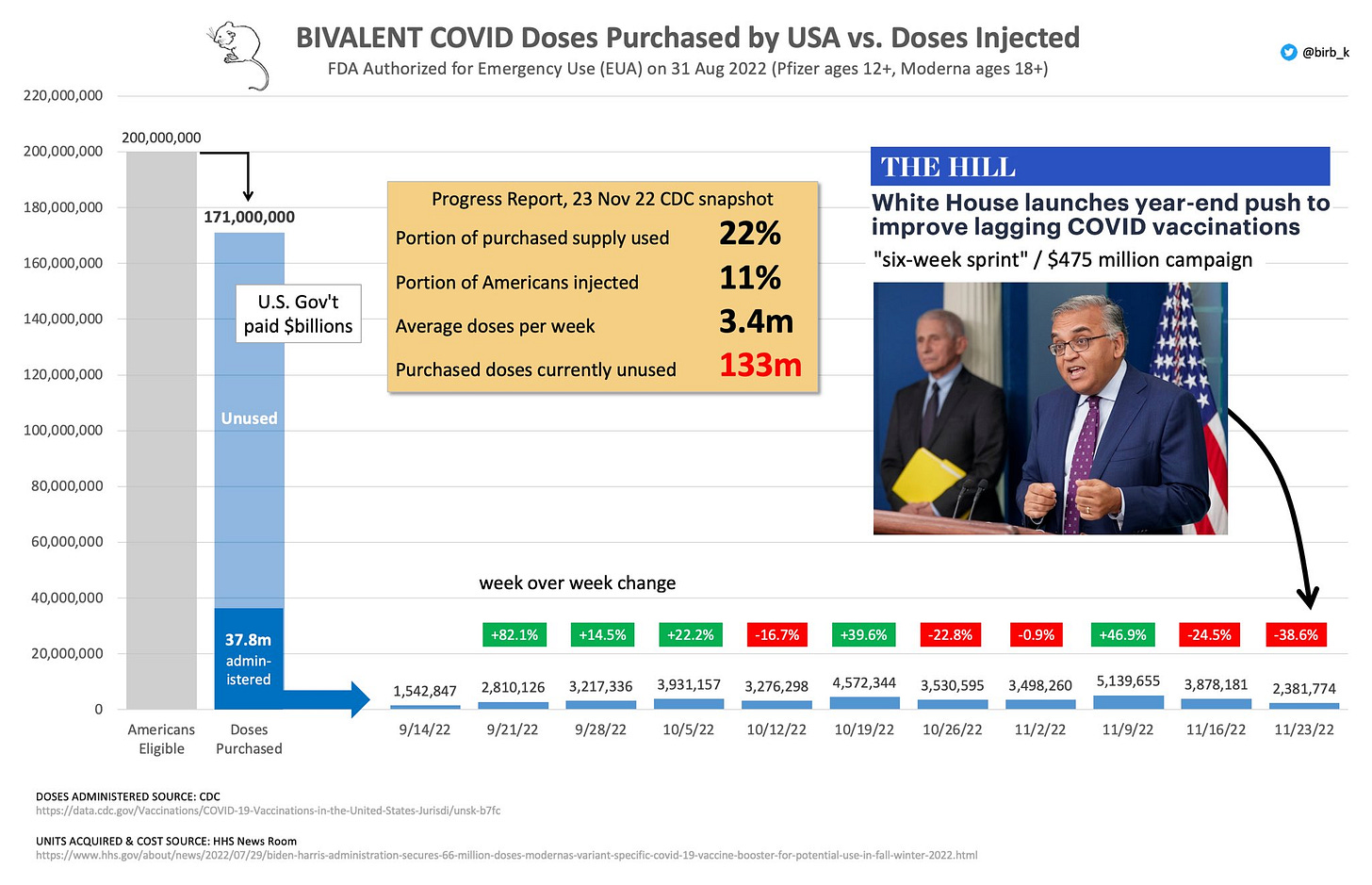
Yet, only 12 percent of Americans 5 and older have received the updated booster. Meanwhile, just over 30 percent of senior citizens — the most have gotten the bivalent dose. In attempts to increase vaccine uptake, the Biden administration has announced a six-week campaign budgeting more than $475 million to expand mRNA vaccine outreach. $350 million will go into community health centers to promote booster awareness while another $125 million will be devoted “to national organizations that serve people with disabilities and older adults to support community vaccination programs and efforts.”
Instead of spending hundreds of millions of dollars trying to persuade Americans to get a fourth shot they likely don’t need, the authorities ought to take a step back and examine why no one is getting the new booster.
Low bivalent vaccine uptake may, at least in part, stem from the disastrous public launch in September when the new shots were approved on the basis of testing on eight mice. No human data existed at the time, yet the new shots were authorized under the much-abused “emergency use authorization” mechanism. This time, even the media’s most trusted public health experts were expressing concern and skepticism. In an interview with the Wall Street Journal, FDA vaccine advisory member Dr. Paul Offit stated, “I’m uncomfortable that we would move forward—that we would give millions or tens of millions of doses to people—based on mouse data.”
On the concern of safety, it was the CDC and FDA’s responsibility to assure the public that the updated booster didn’t carry significant risks like the primary series. Knowing the alarming prevalence of vaccine myocarditis, convincing tens of millions of healthy men to get the new shot was already a hard sell. As the most robust research (Kaiser Permanente) on vaccine-induced myocarditis shows, roughly 1 in 1,800 young men are injured after the second dose. Long-term effects are unknown, but current studies show over half of vaccine myocarditis patients had an abnormal cardiac MRI and a third were not fully recovered at the three-month check-up.
What reassurance have CDC officials given to those concerned with the most common serious adverse event caused by mRNA vaccination? According to CDC official Dr. Sara Oliver, “We know that the myocarditis risk is unknown but anticipate a similar risk to that seen after the monovalent vaccines.”
A similar risk? About 1 in 2,000 to 1 in 5,000 for men under 40? For a disease with an infection fatality rate of less than 0.035% that only harms obese, severely ill, and immunocompromised people?
Are they serious?
The novel COVID-19 vaccines have already injured an untold number of young, healthy men and women, and the pitch from public health authorities for a second booster shot is “we don’t really know what the risks are.”
If safety concerns remain, perhaps the first round of human data on the bivalent vaccine would show promise. Yet all the latest studies are highly confounded, ambiguous, or otherwise flawed.
Late in September, Moderna published a disappointing study looking at the immune response to an earlier version (BA.1) of the latest shot. While they did find a rise in antibody titers, the bivalent vaccine cohort had a higher number of COVID infections than the original booster cohort. The study sample was so small that definitive conclusions were virtually impossible to make. A few weeks ago, Moderna released newer data in 500 participants showing their bivalent BA.5 booster produced five to six times higher antibody levels than the original strain booster.
Pfizer also released their antibody data for the updated bivalent vaccine, reassuring the public that the mass administration of the bivalent vaccine is a necessary next step in combating COVID-19. As stated in the press release, the “Omicron BA.4/BA.5 neutralizing antibody titers were approximately 4-fold higher for the bivalent vaccine compared to the companies’ original COVID-19 vaccine in individuals over 55 years of age.”
As promising as all this data may have seemed, these findings were far from persuasive. A mere “increase” in antibody titers doesn’t necessarily translate to any sustained protection against infection or severe disease. This is widely agreed upon among mainstream virologists and immunologists. Moreover, Pfizer has conceded there’s “no established correlate of protection” between antibody levels and immunity.
To draw more concrete conclusions, clinical data in the real-world is needed — and the CDC released the first study on bivalent vaccine effectiveness on Nov. 22. Unlike nebulous antibody statistics, this study examined vaccine effectiveness in adults 18 and older. While adults 18 to 49 who had gotten bivalent boosters were 43 percent less likely to be infected than their unvaccinated counterparts, older cohorts were far less protected. Those ages 65 and older were only 22 percent less likely to get sick with COVID-19 than unvaccinated individuals of the same age.
As tangled as these results are, they must be taken with a grain of salt. The authors of the study rightly note the findings should be “interpreted with caution because unvaccinated persons might have different behaviors or a fundamentally different risk for acquiring COVID-19 compared with vaccinated persons.”
“The findings in this study are subject to at least six limitations,” they added.
To make matters worse for the public image of the bivalent vaccine, CDC head Rochelle Walensky has shown in real time how ineffective the latest shot is. Walensky twice tested positive for COVID-19 a month after receiving her bivalent booster shot (the window which should have the “greatest protective effect” according to Dr. Vinay Prasad). She tested negative a few days after her first positive result (October 22), but her symptoms appeared to have strangely rebounded on Oct. 30. In light of the new CDC study, Walensky’s re-infection makes perfect sense: Observed bivalent vaccine effectiveness is less than 30 percent in her age cohort—far from the “90 percent effective” health agencies promised with initial doses of the vaccine.
It is a grim sort of irony to witness the bivalent booster shot utterly fail to provide any long-lasting protection in the head of the public health agency most zealously promoting it.
Putting aside the only remaining, arguable rationale for further boosting (those at higher risk), the FDA and CDC have greenlit the new Omicron booster for kids under 12. Moderna’s booster has been authorized for children 6+ and the Pfizer booster for 5 and older.
As USA Today notes: “The companies have not yet completed clinical trials of the booster in younger children. The FDA decided the change to a bivalent vaccine is not likely to have a different effect or risk profile than the earlier shots.”
For this with any knowledge of the inner-workings of the FDA, this is hardly surprising. The FDA is an incredibly corrupt agency with many conflicts of interest. To illustrate, 4,500 FDA-approved medications are recalled a year, on average. 139 for deadly side effects. Based on these figures, a dozen medications will be recalled this month because they kill people. So why are they FDA-approved?
Perhaps in part because 75% of their drug review funding comes from the biopharmaceutical industry, which allows drug companies to get swiftly expedited reviews and approvals. In fact, 68% of pharmaceutical drugs on the market are approved by the FDA through expedited reviews.
As one can infer, quick approvals means less rigorous testing of safety and efficacy.
The totality of evidence for the bivalent booster shot has failed in persuading the American public to get jabbed again. The updated vaccine should never have been approved on the basis of mouse testing. The studies published after approval (that order should have been in reverse) were hardly reassuring. The only study on vaccine effectiveness shows highly limited protection in the most vulnerable groups.
In response to Joe Biden’s tweet urging Americans to get the updated vaccine ahead of the holidays, Jordan Peterson responded,
“Why is the president of the United States shilling for the pharmaceutical industry? Because that’s exactly what this is…”
The answer is quite simple. The Biden administration has ambitiously purchased 170 million bivalent vaccine doses and over 120 million remain unused. Americans have roundly rejected it and moved on from Covid.
The administration may spend millions of tax-payer money promoting the new shot, but until vaccine standards are improved, “emergency” powers are left alone for real public health crises, and the White House COVID response team comes clean on the real dangers and uncertainties surrounding mRNA vaccines, institutional trust may never recover.
The evangelical, evidence-free promotion of highly experimental vaccines — and their new “bivalent” updated iterations — with known safety concerns has destroyed the reputation and credibility of the Biden administration’s COVID response team. I find myself agreeing with (pro-vaccine and mainstream) epidemiologist Dr. Vinay Prasad’s bold assertion:
[The White House] need to fire all their advisors and start new. That’s the only way to fix the situation.
Rav Arora is a 21-year-old, independent journalist formerly writing for top publications such as The Globe and Mail and New York Post before critically covering vaccines and government mandates. Please consider supporting his fearless journalism, focusing on tragic stories of vaccine myocarditis, by becoming a paid subscriber. Read his in-depth vaccine myocarditis series here.



