A Colossal Failure Around the World
Let’s summarize what we now know of the negative efficacy of the COVID-19 vaccines, and why vaccinated people—not the unvaxxed—suffer frequent bouts of COVID-19.
The COVID-19 vaccines—and the new bivalents, of which they are a part—are alarmingly and irredeemably unsafe, as well as ineffective for the advertised purposes. It is increasingly recognized by laypeople, physicians, and scientists throughout the world that the COVID-19 vaccines are neither safe, nor effective, nor reversible.
In this article, I show irrefutable proof that the COVID-19 vaccines are irredeemably ineffective. (See many dozens of my other Substack articles, and my book, “Neither Safe Nor Effective,” on how dangerous these vaccines are.)
U.S. mortality data at the end of 2020 did not support the allegation of a pandemic, because there was no more of an outlying peak in excess deaths in 2020 than other peaks throughout the past two decades, as reported at that time. A series of CDC [Centers for Disease Control and Prevention] revisions have continually increased the number claimed dead in 2020. Even now, as of April 24, the CDC shows that 3,383,729 people died from all causes in the United States in 2020 on one page written in December 2021, [1]
 https://www.cdc.gov/nchs/data/databriefs/db427.pdf
https://www.cdc.gov/nchs/data/databriefs/db427.pdfand also claims that 3,390,079 people died from all causes in the United States in 2020 on a different page.
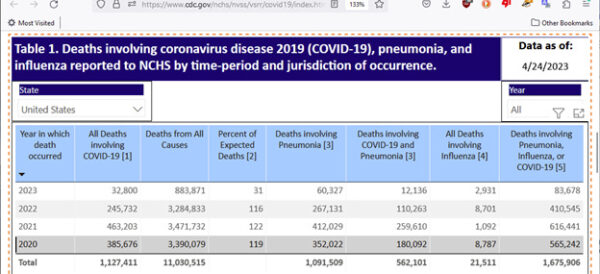 https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htmIf even two years after the end of 2020, allegations of the number of those dead in 2020 continue to increase, at what point will that number be settled? How is it that by December 2021 an accurate number of deaths in 2020 was not available to the CDC?
In either case, mortality for 2020 (the year of COVID-19 virulence) was less than for 2021 (the year of the COVID-19 vaccine), which was 3,464,000. [2] The 2020 mortality number remained at about one percent of the total U.S. population, as in each of the previous three years, in which there was no pandemic.
Notably, December 2020 had by far the highest deaths of any month in 2020 in the United States, 32 percent higher than the average of the previous 11 months of what had been advertised to be the worst pandemic in a century, but in fact had no more than typical numbers of deaths in the U.S. during that alleged pandemic.
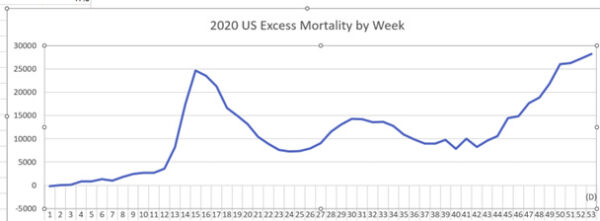
Data released by the Organization for Economic Cooperation and Development show that each of those last three weeks in December 2020, excess deaths (number of deaths over those expected) had higher excess deaths than any of the previous weeks of the alleged pandemic. [3] Each of those last three weeks of December 2020 exceeded 25,000 excess deaths per week, whereas even the worst COVID-19 hospitalization weeks, the first two weeks of April 2020, did not exceed 25,000 excess deaths per week.
The Pfizer vaccines were released to the American public on Dec. 14, 2020. [4]
As of this time, no children are known to have died in the United States with a COVID-19 diagnosis except for those having terminal leukemia and other advanced cancers and grave terminal illnesses and other non-COVID-19 life-threatening circumstances. It has been calculated that seasonal flu, lightning, and being a passenger in a motor vehicle are all more life-threatening to children and adolescents than any of the COVID-19 variants.
It may be no coincidence that December 2020 was the month that the vaccines became available to the public. Early 2021 showed striking excess deaths, and the COVID-19 vaccine was the new factor. Furthermore, January to November 2020 show an average of 274,000 deaths in the United States per month, but since December 2020, according to the same CDC tables of data, the average deaths per month jumped to 288,250.
The Pfizer COVID-19 vaccines first became available for mass vaccination in the United States on Dec. 14, 2020, followed by the Moderna vaccine a few days later. The Johnson & Johnson vaccine would not become available till Feb. 27, 2021. As soon as the earlier vaccines became distributed en masse, the total number of deaths per week for the rest of 2020 from all causes in the United States jumped from 63,000 to 84,000, which is a 32 percent increase, unlikely to be attributable to any other cause but the vaccines. Before the officially reported numbers change yet again, let’s take a screenshot from the CDC.
 CDC National Center for Health Statistics. National Vital Statistics System. Monthly and 12 month-ending number of live births, deaths, and infant deaths: United States. https://www.cdc.gov/nchs/nvss/vsrr/provisional-tables.htm
CDC National Center for Health Statistics. National Vital Statistics System. Monthly and 12 month-ending number of live births, deaths, and infant deaths: United States. https://www.cdc.gov/nchs/nvss/vsrr/provisional-tables.htm Notice how much higher January 2021 deaths are than for each of the next five months. Although January is typically the month with highest deaths in most years, January’s death rate was 32 percent higher than February’s.
It can be seen from the CDC data, that the deaths per week in the United States in each of the first seven weeks following the Pfizer and Moderna rollout all exceeded even the deadliest weeks of 2020 (the two weeks ending April 11 and April 18 of 2020). [5] This should be enough to make anyone hesitant about the vaccines, and logically, more fearful of the vaccines than of COVID-19.
Public Health ‘Experts’ Have Not Been Straightforward With the Data
A confounding factor for assessing safety or efficacy of the COVID-19 vaccines has been a deceptive use of the word “unvaccinated” by the U.S. Centers for Disease Control and Prevention to not only include those who were never COVID-19-vaccinated but also those who have received a dose of a COVID-19 vaccine less than seven or 14 days ago. This “case-counting window bias” allows infections, injuries, and deaths immediately following vaccination to be assigned to, and sometimes even attributed to, the “unvaccinated” category, by deceptive sleight of hand.
Fung, Jones, et al. write of such deception: “This asymmetry, in which the case-counting window nullifies cases in the vaccinated group but not in the unvaccinated group, biases estimates.” [6] A problem with this miscategorization is that injuries and deaths have all peaked closely following COVID-19 vaccination—mostly on the first day—as in the graph below. Yet those individuals, for being so recently vaccinated, are falsely assigned the label “unvaccinated,” confounding much of the reported data.
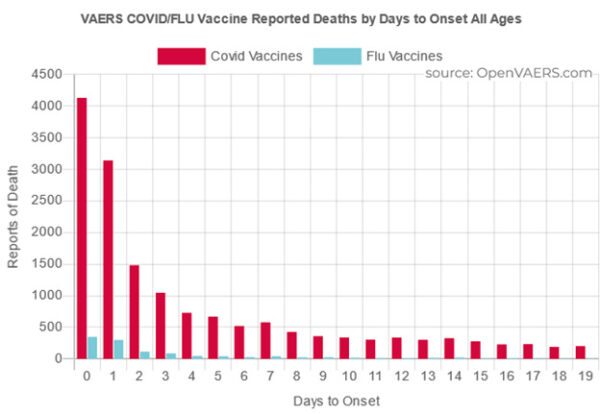 https://openvaers.com/covid-data/mortality
https://openvaers.com/covid-data/mortalityThe only good about this mis-categorization problem is that it is no longer such an issue now in 2023 and going forward. This deception really confounded much data in 2021, the year of peak COVID-19 vaccine uptake, and to a much lesser extent in 2022.
Now in 2023, very few individuals are still being COVID-19-vaccinated, so nearly everyone has made their decision to be vaccinated or not, more than 14 days ago, and are therefore now in widely agreed upon and accurate categories at this late time. But there is little likelihood at this point of eventual correction of previous miscategorization—and therefore corruption—of this essential public health data, 2020 through 2022.
COVID-19 Vaccines Have Negative Efficacy, and What That Means
The COVID-19 vaccines are so ineffective against COVID-19 that they have negative efficacy. This means that you have a greater likelihood of infection and/or hospitalization from COVID-19 after having received the vaccine than not receiving it. The COVID-19 vaccines have not only failed to reduce cases and hospitalizations from Omicron and COVID-19 generally, but they have actually increased the incidence of both. Results of negative efficacy of the COVID-19 vaccines are seen all over the world.
Neither the Pfizer nor Moderna clinical trials addressed preventing transmission.
Tal Zaks is the chief medical officer at Moderna. He told the British Medical Journal, “Our trial will not demonstrate prevention of transmission, because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.” [7]
Dr. Larry Corey oversaw the National Institutes of Health COVID-19 vaccine clinical trials. He said on Nov. 20, 2020: “The studies aren’t designed to assess transmission. They don’t ask that question, and there’s really no information on this at this point in time.” (The article where he was quoted as saying this had not been, but is now, behind a paywall.) [8]
Negative Efficacy Shown by the Most Prestigious Medical Journals
The New England Journal of Medicine shows that those who are fully vaccinated and boosted against COVID-19 recover significantly more slowly from the illness and remain contagious for longer periods of time after SARS-CoV-2 infection. [9]
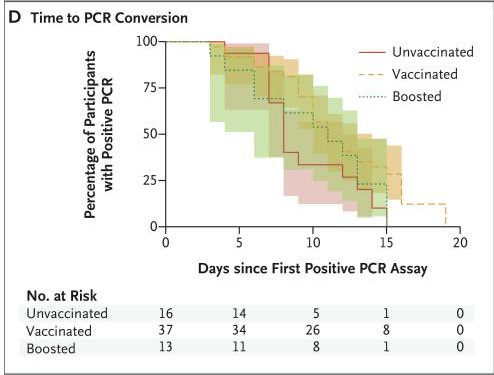 From Figure 1, J Boucau and C Marino, Duration of shedding of culturable virus in SARS-CoV-2 Omicron (BA.1) infection. Jun 29, 2022. N Eng J Med. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9258747/
From Figure 1, J Boucau and C Marino, Duration of shedding of culturable virus in SARS-CoV-2 Omicron (BA.1) infection. Jun 29, 2022. N Eng J Med. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9258747/The Journal of the American Medical Association (JAMA) published data showing that persons receiving two or more doses of COVID-19 vaccines experienced more re-infections with COVID-19 than people receiving 0 to 1 dose and that the probability of reinfection increased with time. “Surprisingly, 2 or more doses of vaccine were associated with a slightly higher probability of reinfection compared with 1 dose or less.” [10]
An analysis in the British Medical Journal found a “net expected individual harm” from the COVID-19 vaccines in the context of college mandates, and calculated that “boosting young adults with BNT 162b2 [BNT162b2 is a lipid nanoparticle–formulated, nucleoside-modified RNA vaccine that encodes a prefusion stabilized, membrane-anchored SARS-CoV-2 full-length spike protein] could cause 18.5 times more SAEs [significant adverse events] per million (593.5) than COVID-19 hospitalizations averted (32.0).” And “for each hospitalization averted we estimate approximately 18.5 SAEs and 1430-4626 disruptions of daily activities—that is not outweighed by a proportionate public health benefit.” [11]
Negative Efficacy of the COVID Vaccines Is Seen Throughout the World
Subramanian and Kumar examined COVID vaccination across 68 countries and found “… the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.” [12]
Switkay showed that Subramanian and Kumar’s trend line regarding relation between new COVID-19 cases and vaccination is not only positive but “… indeed, there is a very strong positive association.” [13]
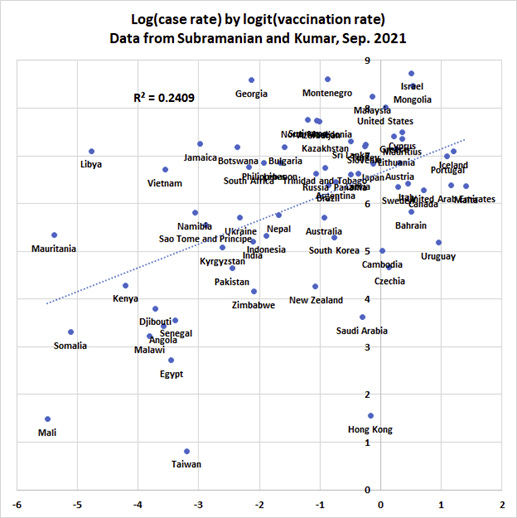 H Switkay. Comment on Subramanian and Kumar… Mar 13, 2022. PDMJ. https://pdmj.org/papers/Comment_on_Subramanian_and_Kumar
H Switkay. Comment on Subramanian and Kumar… Mar 13, 2022. PDMJ. https://pdmj.org/papers/Comment_on_Subramanian_and_KumarA Bayesian analysis of data from 145 countries shows that the COVID-19 vaccines cause more COVID-19 cases per million and more COVID-19-associated deaths per million over the vast international scope of this study. [14] The study found “a marked increase in both COVID-19 related cases and death due directly to a vaccine deployment …” The results in the United States were 38 percent more cases per million [15] and 31 percent more deaths per million [16] caused by the COVID-19 vaccines.
Other studies found no difference in viral loads or rates of infection between vaccinated and unvaccinated. [17] [18] [19]
In order to further comprehend this vast worldwide lack of efficacy of the COVID-19 vaccines, let’s now look at analyses of the phenomenon of negative efficacy of the vaccines in specific countries.
A study of 51,011 employees of the Cleveland Clinic in the United States was done. It found the “Risk of COVID-19 increased with time since the most recent prior COVID-19 episode and with the number of vaccine doses previously received.” [20]
The following graph shows increasing cumulative incidence of COVID-19 disease starting after the first day of the Cleveland Clinic study. We can see a clear dose-dependent increase in infections made worse by each successive dose of the COVID-19 vaccines, with the unvaccinated having far less COVID-19 disease than their vaccinated co-workers.
The small print at the right says, going down from the top [in yellow] more than 3 doses. [in blue] 3 doses, [in green] 2 doses, [in red] one dose, [in black] 0 doses.
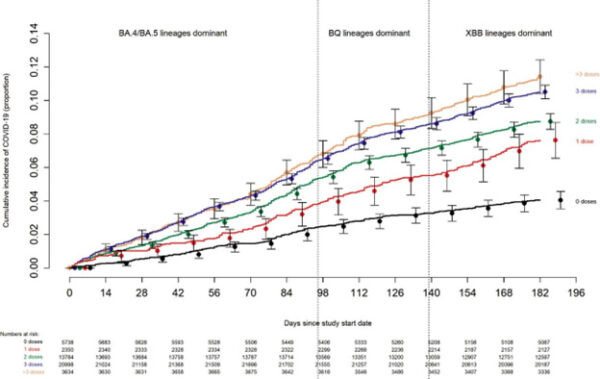 N Shrestha, P Burke, et al. Effectiveness of the coronavirus disease 2019 (COVID-19) bivalent vaccine. Dec 19, 2022. “Cumulative incidence of COVID-19 [infections] for subjects stratified by the number of COVID-19 vaccine doses previously received. Day zero was 12 September 2022, the day the bivalent vaccine began to be offered to employees. Point estimates and 95% confidence intervals are jittered along the x-axis to improve visibility.” https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full.pdf
N Shrestha, P Burke, et al. Effectiveness of the coronavirus disease 2019 (COVID-19) bivalent vaccine. Dec 19, 2022. “Cumulative incidence of COVID-19 [infections] for subjects stratified by the number of COVID-19 vaccine doses previously received. Day zero was 12 September 2022, the day the bivalent vaccine began to be offered to employees. Point estimates and 95% confidence intervals are jittered along the x-axis to improve visibility.” https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full.pdf An Oxford University study of 900 hospital staff members in Vietnam showed that peak viral loads among the infected vaccinated (“breakthrough” infected) staff were 251 times higher than those of unvaccinated personnel. [21]
This Danish study [22] showed that both Pfizer and Moderna COVID-19 vaccines showed negative efficacy against the Omicron variant within only 90 days of administration and that that decline in efficacy was even faster for Omicron than for the earlier Delta variant. This sharp decline is illustrated in the following graph.
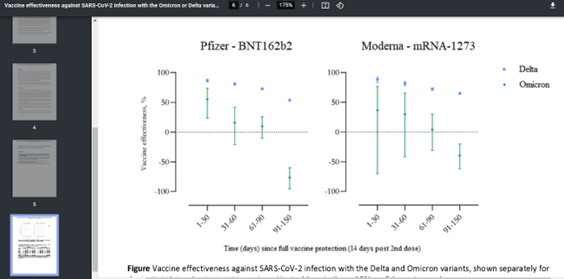 C Hansen, A Schelde, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdf
C Hansen, A Schelde, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdfThe above graph shows that both of the mRNA COVID-19 vaccines predispose toward increased risk for Omicron infection, as the timeline passes the 90-day point, due to negative efficacy.
89.7 percent of people infected with Omicron in Denmark were either “fully vaccinated” or had their first booster. 77.9 percent of the Danish population was fully vaccinated as of the time of the study. [23] Therefore, the vaccinated have been more predisposed to Omicron infection than the unvaccinated in Denmark.
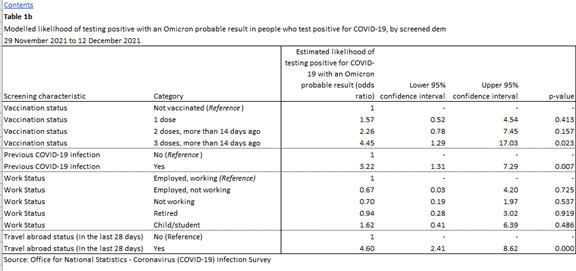
Data from the UK government, Office for National Statistics, shows that each successive vaccine dose has increased the likelihood of testing positive for the Omicron variant, in a stunning display of negative vaccine efficacy. [24]
Worse yet, risk of death from COVID-19 is shown to increase with each successive dose of vaccine for most age groups, as in the following table published by the UK government’s Health Security Agency. [25]
 UK Health Security Agency. COVID-19 vaccine surveillance report. Week 9. Mar 3, 2022. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1058464/Vaccine-surveillance-report-week-9.pdf
UK Health Security Agency. COVID-19 vaccine surveillance report. Week 9. Mar 3, 2022. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1058464/Vaccine-surveillance-report-week-9.pdfOn a population-wide level in Ireland, mass vaccination is correlated in timing with dramatically rising COVID-19 cases. The Irish population has had among the highest rates of vaccine penetration in its adult population, 94.8 percent fully vaccinated as of Jan. 22, 2022, yet COVID-19 cases rose 317 percent over the previous January before the vaccines were in use. [26]
In Scotland also, among those who had received one, two, or three vaccines, or none at all, the unvaccinated had the lowest case rates in January 2022 of all four groups, as seen in this table [27] and graph. [28]
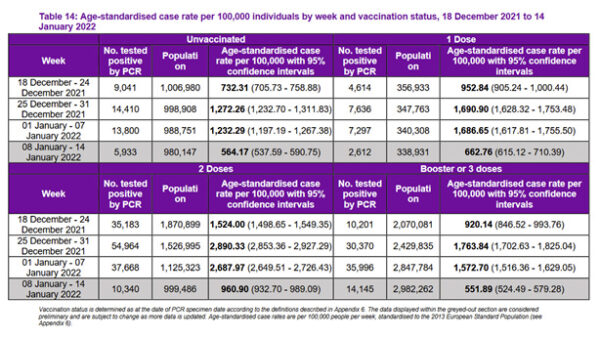 Public Health Scotland. Public Health Scotland COVID-19 & Winter Statistical Report. Jan 17, 2022. p. 38. https://publichealthscotland.scot/media/11802/22-01-19-covid19-winter_publication_report_revised.pdf
Public Health Scotland. Public Health Scotland COVID-19 & Winter Statistical Report. Jan 17, 2022. p. 38. https://publichealthscotland.scot/media/11802/22-01-19-covid19-winter_publication_report_revised.pdf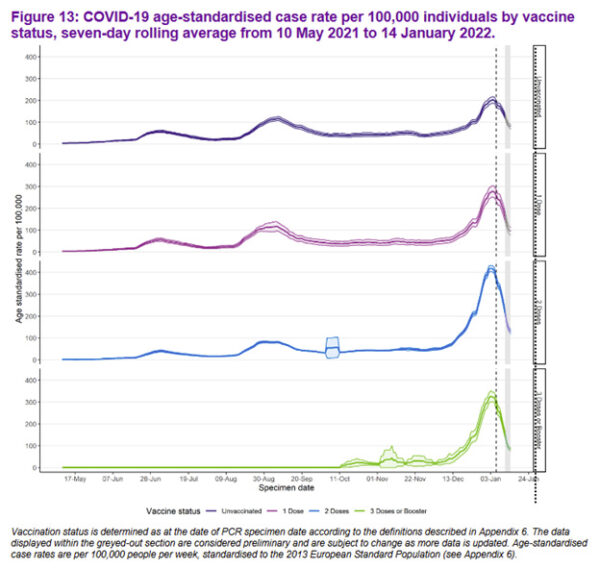 Public Health Scotland. Public Health Scotland COVID-19 & Winter Statistical Report. Jan 17, 2022. p. 40. https://publichealthscotland.scot/media/11802/22-01-19-covid19-winter_publication_report_revised.pdf
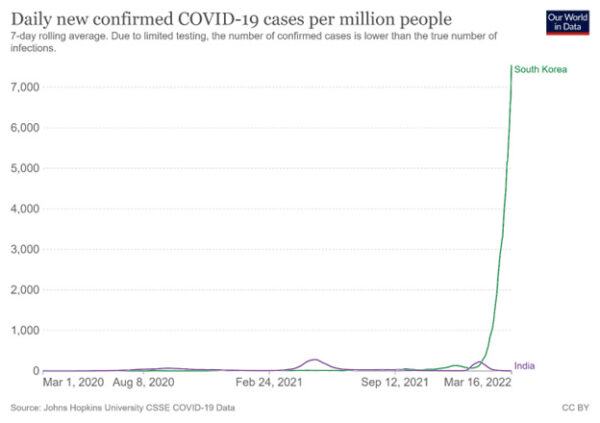
Public Health Scotland. Public Health Scotland COVID-19 & Winter Statistical Report. Jan 17, 2022. p. 40. https://publichealthscotland.scot/media/11802/22-01-19-covid19-winter_publication_report_revised.pdfTwo other very heavily vaccinated countries saw their case rates skyrocket following mass vaccination. Here are South Korea and Germany: [29]
 Johns Hopkins University. Our World in Data. https://ourworldindata.org/coronavirus#explore-the-global-situation
Johns Hopkins University. Our World in Data. https://ourworldindata.org/coronavirus#explore-the-global-situation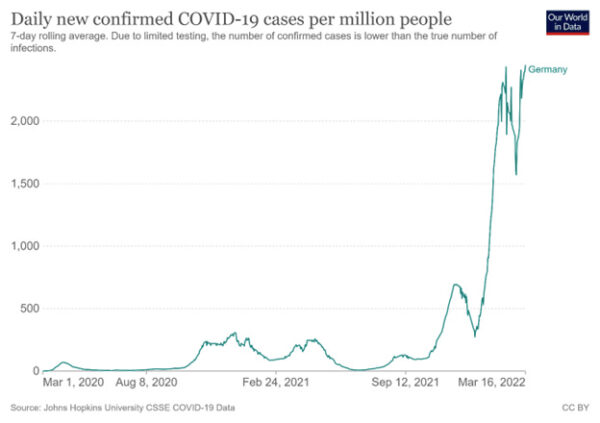 Johns Hopkins University. Our World in Data. https://ourworldindata.org/coronavirus#explore-the-global-situation
Johns Hopkins University. Our World in Data. https://ourworldindata.org/coronavirus#explore-the-global-situationA study of 4,020 cases of Omicron in Germany on Dec. 31, 2021, showed that of those, 1,137 were boosted. There were only 1097 unvaccinated Omicron cases. [30] [31]
However, there are similar numbers of people in the three categories of “boosted,” fully vaccinated” and “unvaccinated” in Germany as of Dec. 31, 2021. German scientists studying the German government’s excess mortality data observed that the higher the vaccination rate, the higher the excess mortality. [32]
As we can see, the unvaccinated have had a strong advantage against Omicron, which was the prevalent COVID-19 strain throughout the world at that time. The COVID-19 vaccines do not work against the Delta strain either. In July 2021, in the United States, in Massachusetts, at a time and place that Delta was predominant, of a total of 469 new COVID-19 cases, 346 of those (74 percent) were in people who were partially or fully vaccinated, and 274 of the vaccinated were symptomatic. [33]
In Delhi, India, of 34 Omicron cases at a hospital, 33 were fully vaccinated (97 percent). However, India’s COVID-19 vaccination rate was only 40 percent at that time. [34]
Both Pfizer and Moderna vaccines were found to plunge to negative efficacy within months. [35] [36] [37]
The Implications of Negative Efficacy in a Heavily Jabbed World
A study by Chemaitelly et al. in Qatar of over 2,000,000 people, for whom vaccination status and COVID-19 disease incidence data were available, showed, just as the preceding studies, that zero to negative efficacy was apparent within months after injection. Authors attributed that decline to “immune imprinting compromising protection in people who had the booster vaccination against the newer omicron sublineages.” The authors explain the mechanism further as [the booster] “could have trained the immune response to expect a specific narrow pre-omicron challenge; thus the response was suboptimal when the actual challenge was an immune-evasive omicron subvariant.” [38]
OAS is likely exacerbated by the mistaken approach of vaccinologists, tampering with the blood, whereas the body is well-prepared to confront new microbes by way of the respiratory tract, not by way of first introduction through the blood.
If the COVID-19 vaccines merely predisposed one to higher risk of the common cold now known as the Delta and Omicron and subsequent variants, then we might simply laugh off these vaccines as a frivolous and superstitious activity. However, the safety data are nothing less than horrifying.
Reposted from Colleen Huber’s Substack.
◇ References:
[1] U.S. Centers for Disease Control and Prevention. NCHS Data Brief No 427. Mortality in the United States, 2020. December 2021. https://www.cdc.gov/nchs/data/databriefs/db427.pdf
[2] U.S. Centers for Disease Control and Prevention. National Vital Statistics System. State and national provisional counts. Monthly and 12-month ending number of live births, deaths, and infant deaths: United States. https://www.cdc.gov/nchs/nvss/vsrr/provisional-tables.htm
[3] Organization for Economic Co-operation and Development. OECD Stat. Health, COVID-19 health indicators, Excess deaths per week, 2020-2023. https://stats.oecd.org/index.aspx
[4] BBC. COVID-19: First vaccine given in U.S. as rollout begins. Dec. 14, 2020. https://www.bbc.com/news/world-us-canada-55305720
[5] U.S. Centers for Disease Control and Prevention. National Vital Statistics System. State and national provisional counts. Monthly and 12-month ending number of live births, deaths, and infant deaths: United States. https://www.cdc.gov/nchs/nvss/vsrr/provisional-tables.htm
[6] K Fung, M Jones, et al. Sources of bias in observational studies of COVID-19 vaccine effectiveness. Mar 26, 2023. J Eval in Clin Practice. https://onlinelibrary.wiley.com/doi/10.1111/jep.13839
[7] P Doshi. Will COVID-19 vaccines save lives? Current trials aren’t designed to tell us. Oct. 21, 2020. British Medical Journal. 371. https://www.bmj.com/content/371/bmj.m4037
[8] A Ault. Can a COVID-19 vaccine stop the spread? Good question. Nov. 20, 2020. Medscape. https://www.medscape.com/viewarticle/941388
[9] J Boucau, C Marino. Duration of shedding of culturable virus in SARS-CoV-2 Omicron (BA.1) infection. Jun 29, 2022. N Eng J Med. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9258747/
[10] E Eythorsson, H Runolfsdottir, et al. Rate of SARS-CoV-2 reinfection during an omicron wave in Iceland. Aug. 2022. JAMA Netw Open. 5 (8). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9350711/
[11] K Bardosh, A Krug, et al. COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities.Dec. 5, 2022. BMJ J Med Ethics. https://jme.bmj.com/content/early/2022/12/05/jme-2022-108449
[12] S Subraminian, A Kumar. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. Sept. 30, 2021. Eur J Epidemio. 36 (12) 1237-1240. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8481107/
[13] H Switkay. Comment on Subramanian and Kumar, “Increases in COVID-19 are unrelated to levels of vaccination.” Mar 13, 2022. PDMJ. https://pdmj.org/papers/Comment_on_Subramanian_and_Kumar
[14] K Beattie. Worldwide Bayesian causal impact analysis of vaccine administration on deaths and cases associated with COVID-19: A big data analysis of 145 countries. Preprint. Nov. 15, 2021. https://drive.google.com/file/d/1DLlRa9rUqvW9pG1vNEsWMEydWwsmSMbe/view
[15] Ibid Beattie. p 41.
[16] Ibid Beattie. p 39.
[17] K Riemersma, B Grogan, et al. Vaccinated and unvaccinated individuals have similar viral loads in communities with a high prevalence of the SARS-CoV-2 variant. July 31, 2021. https://www.medrxiv.org/content/10.1101/2021.07.31.21261387v1.full.pdf
[18] C Brown, J Vostok, et al. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings, Barnstable County, Massachusetts, July 2021. Aug 6, 2021. MMWR Morb Moral Wkly Rep. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8367314/
[19] C Acharya, J Schrom, et al. No significant difference in viral load between vaccinated and unvaccinated, asymptomatic, and symptomatic groups when infected with SARS-CoV-2 Delta variant. Oct 5, 2021. https://www.medrxiv.org/content/10.1101/2021.09.28.21264262v2.full.pdf
[20] N Shrestha, P Burke, et al. Effectiveness of the coronavirus disease 2019 (COVID-19) bivalent vaccine. Dec. 19, 2022. https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full.pdf
[21] N Chau, N Ngoc. Transmission of SARS-CoV-2 Delta variant among vaccinated healthcare workers, Vietnam. Oct 11, 2021. The Lancet. https://papers.ssrn.com/sol3/papers.cfm?abstract id=3897733
[22] C Hansen, A Schelde, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdf
[23] Status of the SARS-CoV-2 variant Omicron in Denmark. COVID-19 Omicron variant report. Dec 31, 2021. Statens Serum Institut. https://files.ssi.dk/covid19/omikron/statusrapport/rapport-omikronvarianten-31122021-ct18
[24] Office for National Statistics. Coronavirus (COVID-19) infection survey, UK: Characteristics related to having an Omicron compatible result in those who test positive for COVID-19. Dec. 21, 2021. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/adhocs/14107coronaviruscovid19infectionsurveyukcharacteristicsrelatedtohavinganomicroncompatibleresultinthosewhotestpositiveforcovid19
[25] UK Health Security Agency. COVID-19 vaccine surveillance report. Week 9. Mar 3, 2022. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1058464/Vaccine-surveillance-report-week-9.pdf
[26] J Horgan-Jones. The Irish Times. Jan. 22, 2022. Total of 100,000 Covid vaccines expire amid slowing demand, Ministers told. https://www.irishtimes.com/news/ireland/irish-news/total-of-100-000-covid-vaccines-expire-amid-slowing-demand-ministers-told-1.4782708
[27] Public Health Scotland. Public Health Scotland COVID-19 & Winter Statistical Report. Jan. 17, 2022. p. 38. https://publichealthscotland.scot/media/11802/22-01-19-covid19-winter_publication_report_revised.pdf
[28] Ibid, Public Health Scotland. p. 40.
[29] Johns Hopkins University. Our World in Data. https://ourworldindata.org/coronavirus#explore-the-global-situation
[30] Robert Koch Institut. COVID-19 in Germany. https://www.rki.de/EN/Home/homepage_node.html
[31] Wochentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19) [article in German] Dec 30 2021. Robert Koch Institut. https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2021-12-30.pdf?__blob=publicationFile
[32] R Steyer, G Kappler. The higher the vaccination rate, the higher the excess mortality. Nov. 16, 2021. https://www.skirsch.com/covid/GermanAnalysis.pdf https://www.utebergner.de/cms/wp-content/uploads/2021/11/%C3%9Cbersterblichkeit-KW-36-bis-40-in-2021-003.docx
[33] G Kampf. COVID-19 stigmatizing the unvaccinated is not justified. Nov. 20, 2021. The Lancet. 398: 10314. P 1871. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02243-1/fulltext
[34] A Dutt. Out of 34 Omicron cases at Delhi hospital, 33 are fully vaccinated. The Indian Express. Dec. 23, 2021. https://indianexpress.com/article/cities/delhi/out-of-34-omicron-cases-at-delhi-hospital-33-are-fully-vaccinated-7686188/
[35] C Hansen, A Schelde, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdf
[36] H Tseng, B Ackerson, et al. Effectiveness of mRNA-1273 against infection and COVID-19 hospitalization with SARS-CoV-2 omicron subvariants: BA.1, BA.2, BA.2.12.1, BA.4 and BA.5. Oct. 1, 2022. https://www.medrxiv.org/content/10.1101/2022.09.30.22280573v1.full.pdf
[37] H Tseng, B Ackerson, et al. Effectiveness of mRNA-1273 against SARS-CoV-2 omicron and delta variants. Jan 8, 2022. medRxiv. https://www.medrxiv.org/content/10.1101/2022.01.07.22268919v1.full.pdf
[38] H Chemaitelly, H Ayoub, et al. Long-term COVID-19 booster effectiveness by infection history and clinical vulnerability and immune imprinting: a retrospective population-based cohort study. Mar 10, 2023. Lancet Infect Dis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10079373/
[39] A Vatti, D Monsalve, et al. Original antigenic sin: A comprehensive review. September 2017. J Autoimmun. 83. https://www.sciencedirect.com/science/article/abs/pii/S0896841117302226?via%3Dihub
[40] A Schiepers, M van’t Wout, et al. Molecular fate-mapping of serum antibody responses to repeat immunization. Jan. 16, 2023. Nature. 615. 482-489. https://www.nature.com/articles/s41586-023-05715-3
[41] D Burnett, R Bull. Total recall? Understanding the effect of antigenic distance on original antigenic sin. March 7, 2023. Immunol and Cell Biol. https://onlinelibrary.wiley.com/doi/10.1111/imcb.12638
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.

