Policy Shifts Against The mRNA Platform Rapidly Emerged This Past Week

Submitted by Steve Z.
Guest Post by Dr. Pierre Kory
Major Covid mRNA policy reversals and awakenings occurred this week within a major U.S health system, a large U.S state, a South American country, and in the UK. The dominoes are starting to fall.

OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER
This week a nurse reached out with disturbing descriptions of some major changes she has witnessed inside the Ohio State University Medical Center (OSUMC) system.
OSUMC s a large and comprehensive healthcare organization, with a significant presence in Ohio and a strong focus on research, education, and patient care. It is a massive institution with over 23,000 employees, including:
- Over 2,000 physicians
- More than 1,000 residents and fellows
- Nearly 5,000 nurses
Lets start off with this screenshot of a webpage from OSUMC’s website which provides information to the public as to where they can get Covid-19 vaccines. Check out the highlighted sentence at the bottom of the page:
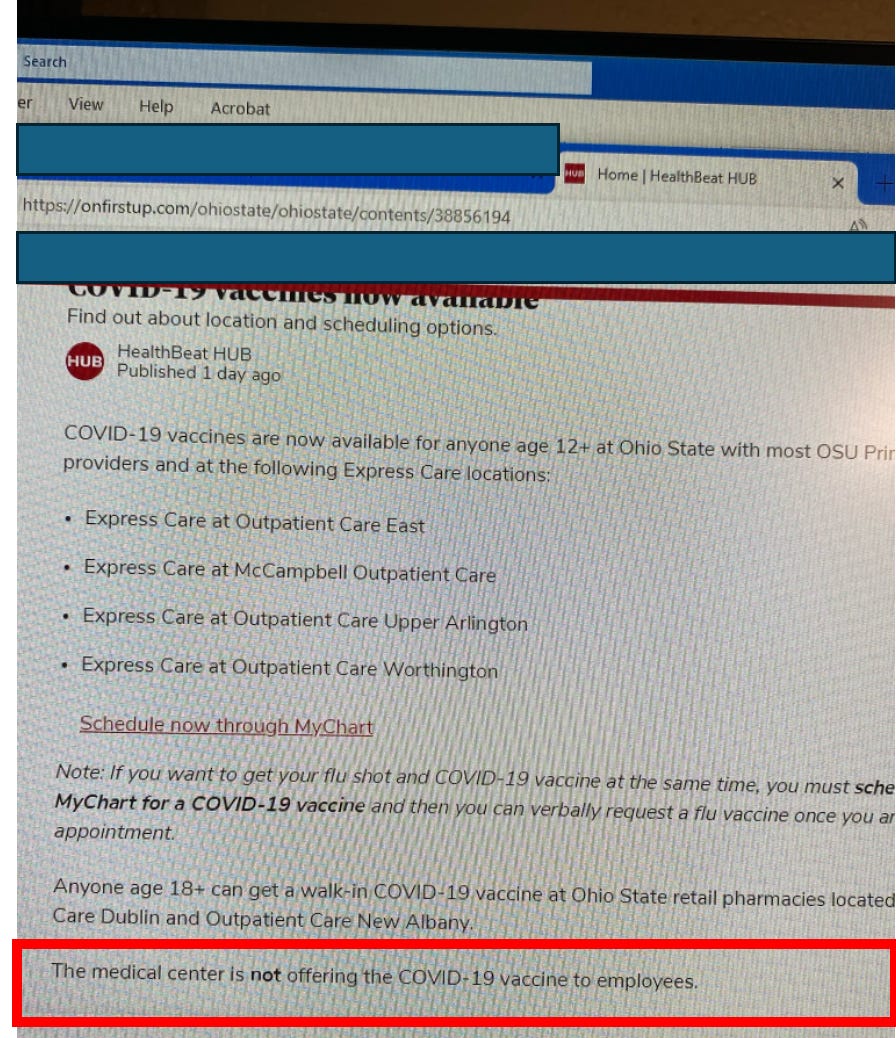
Wait, what? Ohio State is suddenly no longer offering the Covid-19 vaccine to any of their employees but they are happily offering to inject them into the public? How can such a policy be justified? Why was this change in policy done and why was it done so quietly?
Let’s get this straight. Ohio State’s leadership is now making an institutional decision that employees should not be offerred access to any Covid-19 mRNA vaccine. I am (pretending to be) confused. I mean, if the vaccines could protect patients from being infected by staff members and they were safe to give to staff members, why wouldn’t you do everything possible (like a mandate) to ensure they receive them?
The only possible reason for the action above is that either OSUMC leadership recently discovered that the vaccines: a) do not work or b) are not safe. I think you would agree that, of the two possible answers, the only one that makes sense to explain this abrupt change in policy is B) they are not safe. I say this because if they were safe but instead just didn’t really work very well, Ohio State would not have the incentive to divorce themselves so abruptly and strongly from the recommendations of our benevolent federal government. I believe such an action would pretty quickly and negatively impact federal research funding by the NIH. It is my belief that agency’s money kept the nations 126 major academic medical centers in line throughout Covid, as those CEO’s and Deans are well aware that NIH retaliation in terms of rejecting grant funding if they “dissent” is real and happens (inflated reimbursements from the gov’t was another one of course).
I asked the brave browser AI, “why is Ohio State Medical Center no longer offering Covid-19 vaccines to its employees?” Two sentences jumped out:
- “Based on the provided search results, it appears that Ohio State Medical Center did offer COVID-19 vaccines to its employees at one point.”
- “Without further information or clarification from Ohio State Medical Center, it’s difficult to provide a definitive answer on why they may not be offering COVID-19 vaccines to their employees.”
So it must be the case that Ohio State leadership somehow found themselves a stronger financial disincentive to subjecting employees to Covid-19 vaccine injection. Where would such a disincentive come from? Answer: lawsuits. I also suspect that fear of worsening staff shortages from disability and/or death further disrupting operations played a role as well (as you will learn below).
This new policy action (taken very quietly) is absolutely dam breaking to me in terms of progress towards the truth about the mRNA platform getting out to the public. It is also appears ethically reprehensible, i.e. the institution made the decision to keep jabbing the public with a toxic and lethal vaccine while becoming aware that same vaccine is either exposing them to unmanageable legal risks and/or is disrupting their operations by negatively impacting the health of their workforce. Welcome to dystopia.
Next, lets take a “little deeper look under the hood” as to what is going on at OSUMC. I think, after reading the below, it is not an overstatement to say that their system is altering on many levels. I would not want to be a patient there, solely based on what I learned from this nurse. Sorry not sorry OSUMC.
What follows is a para-phrased summary of a long telephone conversation I had with my newest nurse informer. She describes the beginning of a sea change in both perspective and open discussion around the “vaccines” that has occurred within OSUMC over the past 6 plus months. At the same time, she tempers that reality by later noting that many staff still have no ability to associate these changes to the vaccines (even when themselves have fallen ill). Although I can’t take credit for the start of that change in awareness, it is what I have worked tirelessly toward for the past 3 1/2 years. However, hold on to your hats folks because what is happening in hospitals in regards to the quality of medical care right now is downright disturbing.
Here are the most potent pieces of information I gathered, in no particular order:
- An increasingly noticeable number of doctors and nurses and staff have “died suddenly,” “died unexpectedly,” or have become disabled and ill from injuries and/or cancer. The youth and health of these employees have been increasingly remarked on amongst staff (not to mention the deluge of previously healthy and/or young patients they are now presenting with severe and/or atypical (for that age) illnesses. Remember, cancer used to largely be a disease of aging.
- Consequently, the suspected role of the vaccines in most of the deaths is more of an open secret and of growing concern among staff there. To wit, Ohio State University Medical Center (OSUMC) also recently stopped emailing out obituaries of prominent or veteran employees when they die. Why you ask? Because of both the number of them as well as the comments posted by employees that began openly calling out the likelihood that the vaccines were a cause (i.e. they would point out the dates of the decedents vaccination and their death). Unsurprisingly, she also told me OSUMC would quickly censor any posts of that nature (despite containing no foul language, personal attacks, or threats). From a phone conversation we had:
“Yes, this is huge. Lots of internal cases of death and disabilities. They quit posting internal obits for staff. The comments underneath them were showing that people knew why everyone was dropping dead for baffling reasons. So those went away.”
- A number of physicians (the most noticeable of them being superspecialists who cannot be replaced easily), besides dying, are also leaving due to disability or retiring due to health reasons.
- She is hearing of a growing number of lawsuits by family members of these physicians against OSUMC for the mandates which led to the deaths or disabilities.
- One lawsuit was filed by a widow of a physician who dropped dead suddenly. Interestingly, she demanded an autopsy with staining for spike protein and the heart was found “loaded with spike.”
- Outcomes of organ transplant patients have been plummeting since the mRNA campaign. It got so bad that, in a complete reversal from two years ago where the programs had insisted on both donors and recipients getting jabbed, at OHSUMC they apparently no longer require or recommend mRNA vaccines to recipients and may be prioritizing organs from unvaccinated donors. Whoa. Apparently one of the reasons is that recipients were developing new “systemic” conditions that were not typical or expected in transplant patients previously.
- Minutes of administrative and policy committee meetings are no longer openly available on the internal OSUMC website and are instead only available if you “sign in” (presumably so they know who is looking up these minutes).
- When physicians die suddenly, this creates a huge mess operationally due to the fact “open notes” in the electronic medical record (EMR) can’t be closed and the chronic, ongoing care of large numbers of often long time or highly active patients become disrupted. In her words, “dealing with the practice of a doc who died is a mess – dealing with open notes, ongoing patient care, patient calls, and maintaining plans of care.”
- Many of the disabilities and deaths of physicians were discovered by this nurse while she was following up on notes that were “left open” in the EMR. She would then be told by the staff about the injury, death, or disability of the health care provider who started the note. Many of the illnesses or disabilities were described to her as being due to neurological issues – either overt neurological deficits or cognitive decline/impairment and even dementia (AMD comprehensively compiled the data showing the negative cognitive impacts from the mRNA vaccines here). Further, adding the “abandoned” patient panel to healthier and still working physicians in that specialty was causing further strains. This is important because cognitive impairment is one of the most common side effects of the COVID vaccines, something not only shown by the data but also what I bear witness to each day in clinical practice.
- Cancers are exploding, causing massive strain on oncology services. Particularly glioblastomas to the brain as well as to the spine. Also, case managers for the large number of cancer patients were stating they were not retiring due to the patient volume in need.
- Even worse, cancers are being missed at high rates given that the “index of suspicion” in younger patients is not appropriately high enough. As a result, doctors are missing cancers as evidenced by retrospectively “obvious” signs and symptoms in the record.
- Applications for both short and long term disability have risen so much they have created backlogs and delays that staff have noticed and are more openly talking about. The often young ages of the staff applying for disability has not gone unnoticed either.
- She knows of several colleagues either declining or dying from cancer but are forcing themselves to work in order to provide for their family.
[A Midwestern Doctor, who helped me on this story, asked me to note that we both know numerous doctors who have been become impaired or disabled from the COVID vaccines, many of whom then had to enter an early retirement early, and sadly, quite a few others who died prematurely from a vaccine side effect. Many doctors are still in denial about this, but many others are getting red-pilled because the damage is undeniable and can’t be ignored since its directly affecting them—with this newly awakened crowd including many physicians who have begun speaking out about the vaccines and I will discuss in an upcoming article.
The key point AMD wanted to share here is that the COVID vaccines were sold with the most aggressive marketing campaign in history, so every possible tactic which could be used to sell them was. One of these was using healthcare workers as the initial cohort to promote the vaccines since it would be easy to manipulate them into fully vaccinating, the public trusting their endorsement, and them being less likely to publicize the side effects of the shots. Because of this, doctors were some of the most highly vaccinated Americans, and in turn had some of the highest rates of injury. As such, we expect the decline in medical care see in Ohio is not an isolated example.]
Issues Among Nurses, Nurse Practitioners, Case Managers and Physician Trainees
The following reports of the diminished skill levels of new trainees are truly troubling given their likely consequences – they threaten the quality of care we expect to receive in an American hospital. I suspect the growing “fear of hospitals” which began in Covid will not be helped by the following so I apologize in advance:
- Training standards and skill/knowledge levels have noticeably declined as well. She blames this on the younger providers having been trained during Covid with insufficient patient contact/volume and limited face-to-face communications (ipads were overly used to communicate during Covid). The younger nurses and doctors are “terrified of making a decision” due to their lack of knowledge and experience (which I would argue may be a good thing).[AMD asked me to emphasize that many medical trainees had “virtual” rotations during the pandemic or skipped in-person lectures that taught basic doctoring skills during the pandemic and that all the medical educators AMD queried felt this was devastating to the COVID trainees future clinical competency]
- One senior physician specialist was so alarmed with the skill level of his fellows in training that several of them were discharged from the training program. (ED: As a former Director of a pulmonary and critical specialty program for several years and throughout my career at a large teaching hospital, I had only ever had one fellow have to go through “remediation” but he made it to graduation. To not make it through remediation means they were completely unqualified, although, if there were more than one of them, it likely was not their fault that they proved not up to the job).
- In her words, “the senior physician had first made a policy of not allowing first year fellows or residents to be consulted before the attending (Ed: this is not how patient care has traditionally been delivered in a teaching hospital). Several fellows did not make it because they were so bad. They were prevented from seeing patients and this was done abruptly with nobody arguing.”
- New, inexperienced and poorly trained patient case managers are being hired, often working remotely and consistently demonstrate poor knowledge and skill in extracting the relevant and needed information from the records. She often discovers during chart review that the patient has a different problem and needs a different solution. In her words “they are hiring new grads with new certifications, they don’t know shit, cant even pronounce diagnoses correctly, and can’t read a chart. Many are contractors where I don’t know who they are, where they are from, and they don’t know what they are doing…”
- Nurses: “Nurses are dumbed down, know very little, skill sets are poor. Patient errors are up, charting is shitty, typically among the young nurses, basic charting is deplorable compared to new grads in the past. This is occurring despite the electronic medical record being designed to guide your charting… not turning the patients enough, neuro checks are poor, notes have immense copy and pasting with lots of errors, and they are not charting enough.”
- Nurse Practitioners: “The nurse practitioners are not looking at patients, and they are not picking up on patient issues that develop.. They come from “fast track” NP programs with clinical training times that are totally insufficient. They don’t know shit. Plus, the nurses going into NP programs have only a few years of nursing experience (Ed: typically NP’s have extensive nursing experience prior to entering an NP program).
- Now she also emphasized that the problems with nurses and NP’s preceded Covid, “traditional NP programs had required extensive experience in cljnical settings but no longer do so now. It might work if the undergrad programs were in a science-centric major. That is often not the case and it shows.”
- “Covid made it worse by fast tracking for needs rather than assessing for nurses aptitude and reasonable expectation of success for the quality of care a patient receives.”
- “The young nurses are not reading up on their patients enough at beginning of shift. They do not communicate well to other staff in preparation for their patients procedures. Shift report is a garbage-in thing with inexperienced ones. They don’t realize what is truly important to know.”
- She then talked about the mRNA campaign and mandates in context of what she has observed in her career by saying “The other thing I’ve always been aware of and leery of is that we work in a system that does not ensure our exposures to highly dangerous “things” and that is cumulative. I know some cases had to have been due to exposures that were brushed off, but set the body up for disaster once jabs and boosters especially were introduced to the body.”
- When I asked her to be more specific as to what she meant, she replied, “There are often no lead aprons available to protect staff during procedures with radiation exposures. Chemo protocols are ignored – exposure to chemo agents forbidden out of cancer center. Tent/aerosolized chemo on floors that do not have protocols for that. Disregard in bed placement to unit limitations and appropriate staff. Things like that ongoing for many years and I believe is cumulative.”
Now, although some of the above suggests that the staff is “awake,” she tempered against this interpretation with the following statement, “at the same time, many staff do not openly acknowledge or appear to connect illness and disability status, let alone cancers, to “vax” or boosters. Not everyone is clinical, trained, reads and researches. There is still an enormous amount of trust in the System. And most do the traditional treatments for cancer. They do not know of ivermectin, mebendazole, etc. Trust is a hard horse to get off. It’s almost a cult like environment. The cult you never recognize is the one you are in.”
FLORIDA SURGEON GENERAL RECOMMENDS AGAINST THE ENTIRE mRNA PLATFORM
Please contrast the quiet, cravenly change of Covid vaccine policy by Ohio State with that of Florida’s Surgeon General, Joe Ladapo MD, PhD. Joe is someone who has been a colleague of mine during Covid as he had consulted me for my expertise on ivermectin a while back, and more recently someone who I call a friend.
Recall that his first courageous and appropriate federally rebellious policy action occurred back on September 13, 2023, when he provided guidance against COVID-19 boosters for individuals under 65 and younger.” This week, on Thursday, he decided to protect everyone (not just employees and the medical centers) by issuing a strong recommendation against all Covid mRNA vaccines, citing both lack of safety and lack of efficacy. Incredible, ethical, courageous. There is still a “real” physician working in public health. Check it out, from this bulletin posted on Thursday, Florida’s Dept. of Health (FLDOH) wrote:
- FLDOH is reminding health care providers of the importance of remaining up to date with current literature related to COVID-19 vaccines and boosters, and the importance of providing patients with informed consent.
- He then calls out the absurdity of the (P)FDA approval a few weeks ago of the most recent Pfizer and Moderna vaccines given they target the omicron variant “which is not causing a significant number of infections.” Plainspoken. Commonsensical.
- He then reminded the public that no clinical trial data for the boosters was available to support such an approval. He also plainly states that it does not target the current variant which is causing 37% of infections at this time.
- He lands another blow when he wrote, “the federal government has not required COVID-19 vaccine manufacturers to demonstrate their boosters prevent hospitalizations or death from COVID-19 illness.”
- Additionally, “the federal government has failed to provide sufficient data to support the safety and efficacy of COVID-19 boosters, or acknowledge previously demonstrated safety concerns associated with COVID-19 vaccines and boosters, including:
- prolonged circulation of mRNA and spike protein in some vaccine recipients,
- increased risk of lower respiratory tract infections, and
- increased risk of autoimmune disease after vaccination.
And then, in the middle of the bulletin in all bold:
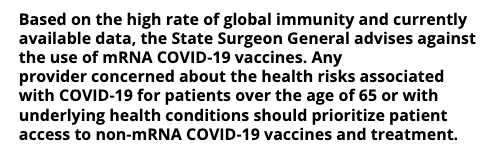
If only the rest of the country’s Surgeon Generals and Health Departments could have put in the work studying the mRNA platform the way Joe and his team did. I see this action as a rebellious ray of sunshine in a bleak, totalitarian public health landscape.
URUGUAY
My dear friend, Dr. Hector Carvallo of Argentina, reached out to me this week because he said that a group of Uruguayan doctors wanted to consult with me and he wanted to know if he could give them my contact. Know that Hector is the “Pierre Kory” of Argentina or more accurately, I am the “Hector Carvallo” of the U.S (or maybe Paul Marik is).
Anyway, of course I said yes, and a doctor who I had previously met with on zoom a couple of years ago wrote to me as follows:
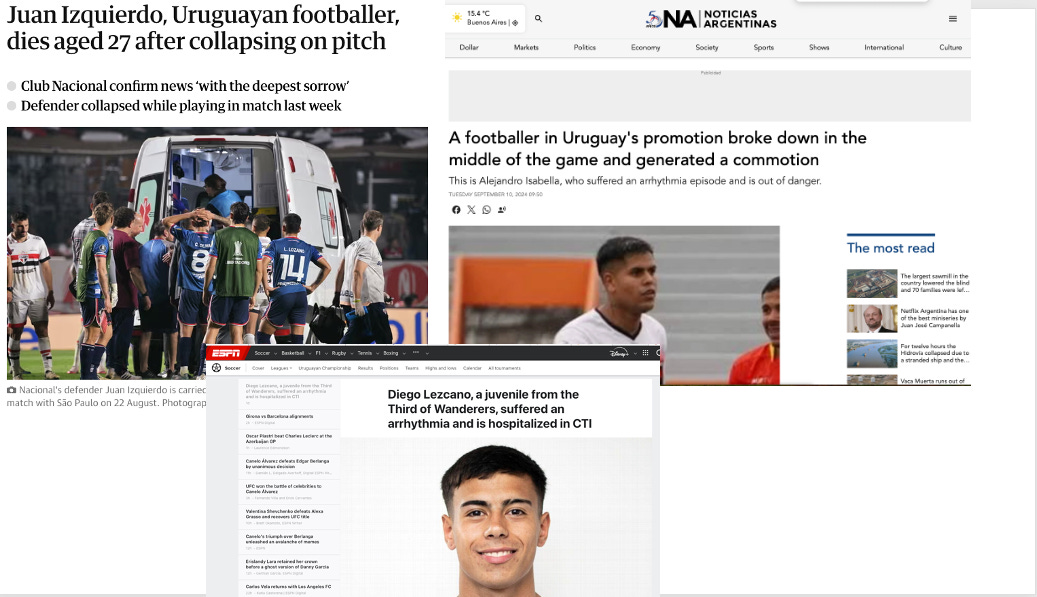
“Hello Dr. Kory, My name is José Arigas, I’m an orthopedic surgeon in Uruguay. I had the chance of talking to you in a zoom meeting two years ago. During the last month our country has witnessed the stories of three soccer players who had cardiac issues, one of whom died. This has been an eye-opening event for people.
I have tried talking to my colleagues but it’s useless, they don’t want to see what is happening. I would like to know if there is any diagnostic approach to prevent sports-related cardiac problems in vaccinated people.I appreciate all the work that you have been doing, giving Medicine the place it deserves.”
I later learned the names of the players: Juan Izquierdo (he died on 8/27/24), Alejandro Isabella (collapsed with an arrythmia on 9/9/24) and Diego Lezcano (suffered an arrythmia at home on 9/11/24). Basically, in just over 10 days, three Uruguayan footballers collapsed or died. Lezcano, who arrested at home is still on a ventilator and was found to have a dilated cardiomyopathy. Three professional soccer players from Uruguay collapsing over a ten day period has apparently started to “awaken” the general public but not the doctors as per Dr. Arigas. Shocker.
All I could do was send him a link to this paper below by Peter McCullough and Nicholas Hulscher where they propose a risk stratification protocol to try to identify vaccinated athletes at risk of a cardiac event.
UK MEDICAL COUNCIL DROPS CASE AGAINST DR. TINA PEERS
Another major, positive event happened this week concerning my friend and colleague, Dr. Tina Peers from the UK. She is an outspoken physician who did early treatment for Covid and called early attention to the harms of the vaccines. Like me, she specializes in treating Long Covid and Long Vax and has become a valuable colleague given her long standing expertise in Mast Cell Activation Syndrome which commonly befalls these patients. Unsurprisingly, her Medical Council accused her of misinformation and not comporting with standards of care etc. However, unlike me who lost my three Board certifications a few weeks ago, her case was.. dropped this week! Apparently, the Council did not have a desire for a public hearing where she was going to call up her vaccine injured patients to testify on her behalf. Perhaps this too might represent the beginning of a sea change in that regulatory authorities will start to end the persecution of expert Covid physicians?
Since COVID started, I’ve been doing everything I can to help get the word out on the dangers of how its been handled and help patients who were hurt by it—which leads to me never being able to get to everything I want to. I sincerely appreciate your support of this Substack and what you’ve made it possible for me to do.
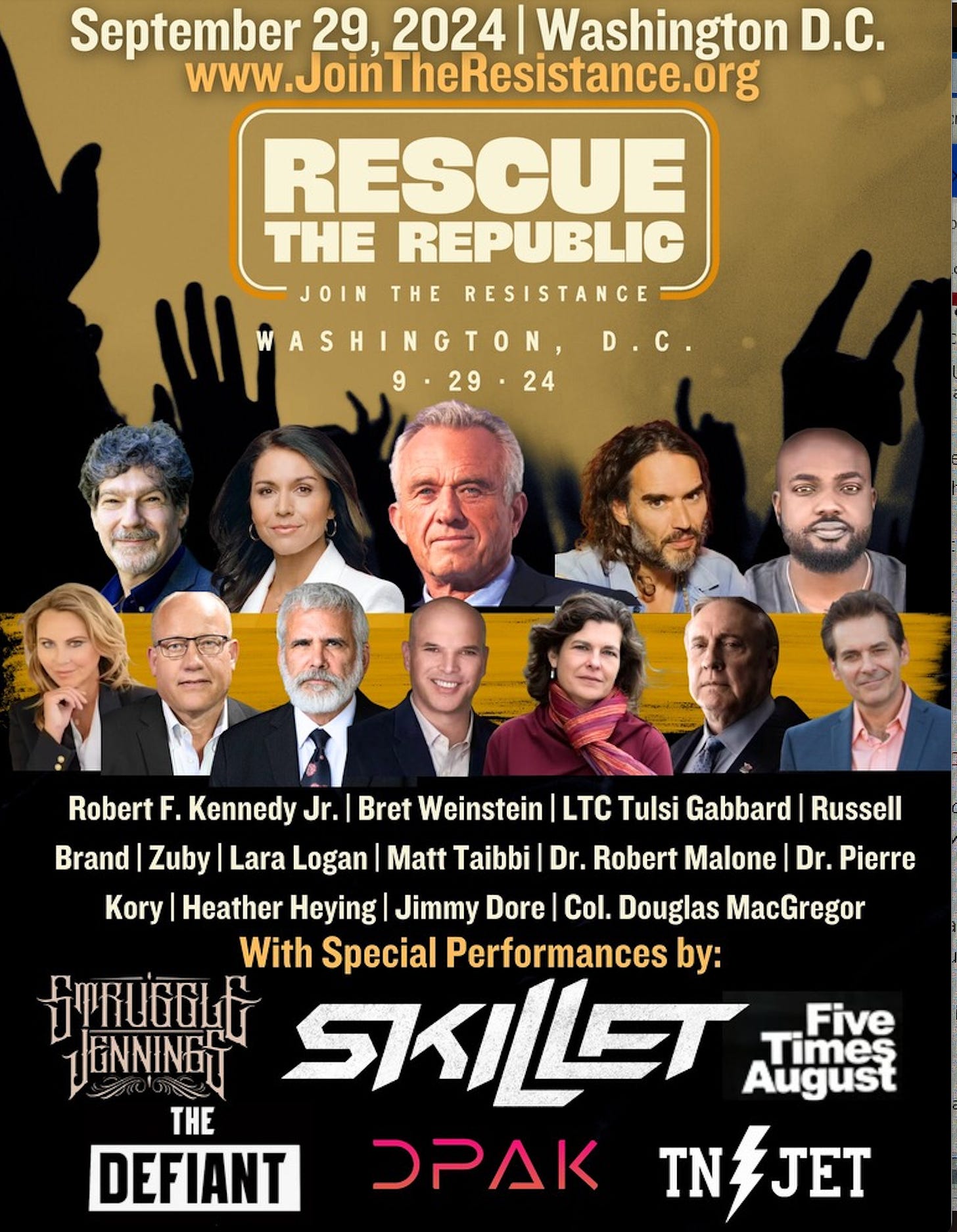
P.S. I truly hope that people will show up and support our big rally called “Rescue the Republic” on Sept. 29, 2024 between the WWII Memorial and the Washington Monument. Join me, RFK Jr, Bret Weinstein, Russell Brand, Jordan Peterson, Matt Taibbi, Lara Logan, Jimmy Dore, Tulsi Gabbard and more See below link:
P.S.S Similar to the above, I previously wrote a series of posts I wrote which I titled “Nursing Reports From The Front Lines Of The Vaccine Catastrophe.” Those posts contained innumerable details of events occurring during the mRNA vaccine campaign within a major health care system which I obtained from a senior, veteran ER/ICU nurse who was fully awakened to the Covid mRNA platform’s dangers. Here are the previous posts if interested: